40 Two-Stage Subpectoral Tissue Expander–Implant Reconstruction
Summary
Tissue expander (TE) reconstruction with partial muscle coverage and acellular dermal matrix (ADM) is the most common means to reconstruct the breast following mastectomy in the United States. The benefits of the procedure include a relatively rapid recovery without donor site morbidity in other areas of the body. Compared to direct-to-implant reconstruction, tissue expansion allows more enhancement in size if desired and a second surgery to make adjustments to the final implant pocket. Although initial reports of TE–ADM reconstruction yielded higher complication rates compared to total muscle coverage when surgeons were learning the technique, more recent studies have demonstrated no difference in complications. Furthermore, the aesthetic outcomes are improved with partial muscle release with more lower pole expansion and a natural breast shape. Compared to prepectoral tissue expansion, there is less upper pole visibility but more animation with pectoralis muscle contraction.
Key Teaching Points
Tissue expander (TE) reconstruction with partial muscle coverage and acellular dermal matrix (ADM) is the most common means to reconstruct the breast following mastectomy in the United States.
The benefits of the procedure include a relatively rapid recovery without donor site morbidity in other areas of the body.
Compared to direct-to-implant reconstruction, tissue expansion allows more enhancement in size if desired and a second surgery to make adjustments to the final implant pocket.
Although initial reports of TE–ADM reconstruction yielded higher complication rates compared to total muscle coverage when surgeons were learning the technique, more recent studies have demonstrated no difference in complications.
The aesthetic outcomes are improved with partial muscle release with more lower pole expansion and a natural breast shape.
Compared to prepectoral tissue expansion, there is less upper pole visibility but more animation with pectoralis muscle contraction.
Surgical Plan
Determine if nipple preserved: nipple-sparing versus skin-sparing versus skin-reducing mastectomy.
Choose incision: optimize access, minimize scar burden, optimize nipple position if preserved.
Choose muscle position: total, partial, or no muscle coverage.
Choose support matrix: Choice of acellular dermal matrix variants and synthetic matrix.
Determine tissue expander style: projection, width, volume, tabs.
Closure: drains and dressings.
Postoperative care: surgical bra, antibiotics, management complications.
40.1 Marking and Preoperative Considerations
The mastectomy may preserve or remove the nipple (▶Table 40.1).
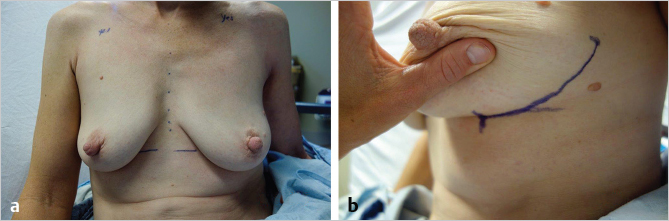
In cases of nipple-sparing mastectomy, a number of access incisions may be considered. The inferolateral inframammary fold (IMF) incision offers an inconspicuous scar and good access for both mastectomy and reconstruction (▶Fig. 40.1, ▶Fig. 40.2). There is a learning curve with the technique, but once mastered, this incision has among the lowest complication rates. The reason for this is likely attributable to the thicker skin as the breast transitions to the abdomen, as well as skin retraction forces directed at a location distant to the nipple itself. A lateral straight or lazy S incision preserves the most blood supply to the nipple and may be the safest choice when first learning nipple-preserving techniques. A periareolar incision superior or inferior to the nipple, with or without a lateral extension, has the advantage of familiarity in technique compared to the skin-sparing mastectomy. When used wisely with a two-stage approach, this incision may be considered and may allow more nipple elevation if an ellipse of skin is excised with superior access. However, it should be noted that anatomically this incision will remove more blood supply to the nipple and it has been associated with a higher rate of nipple necrosis in some series. An inferior vertical incision helps centralize the nipple in large and/or ptotic breasts. This incision places more tension in a horizontal dimension and may limit initial fill.

Clinical Pearl
The inferolateral inframammary fold incision for nipple-sparing mastectomy optimizes cosmesis, while the lateral radial or lazy S incision preserves the most blood supply and may be the safest.
Initial markings prior to the mastectomy include the IMF on bilateral breasts and the overall symmetry in fold location. The lateral border of the breast may be marked to help plan an inferolateral IMF incision.
Tissue expander–implant (TE–I) versus direct-to-implant (DTI) breast reconstruction: In implant-based reconstruction, there are two approaches. A two-stage TE–I reconstruction places a TE at the initial stage in conjunction with the mastectomy. This approach requires exchange to an implant at a later date in a second surgery under general anesthesia. In contrast, if the skin is sufficiently perfused, consideration is given to placing the final implant (DTI) at the time of the mastectomy. There are advantages and disadvantages to each approach (▶Table 40.2).
Clinical Pearl
If the breast skin is sufficiently perfused to place an implant of desired size at the time of mastectomy, direct-to-implant can be considered.
In addition, TE reconstruction may have distinct advantages in patients with asymmetry, ptosis (for optimizing nipple position), and very large breasts (700cc+) for overall implant positioning and tailoring of the skin envelope.
40.2 Tissue Expander Placement
The TE may be placed with total, partial, or no muscle coverage. The most common approach currently is partial muscle coverage with ADM (▶Table 40.3).
40.2.1 Acellular Dermal Matrix
The most common type of ADM in the United States is human. Human ADM has many desirable properties including the ability to be revascularized and integrated into the patient’s body for long-term soft tissue support, pliability and elasticity, strength and durability, and lack of immune response and scarring/contracture. Human ADM serves as the gold standard for which other matrix products are compared. Bovine and porcine ADM are also available and share many of the advantages of human ADM. In attempt to decrease overall costs, many products have been developed including those made from pericardium and synthetic materials such as silk, Vicryl, prolene, and titanium. The challenge of the newer products is in providing the same efficacy, longterm tissue support, lack of scarring/contracture, and biointegration as ADM materials. In synthetic permanent matrix materials, additional concern arises over the ability to remove the material in the presence of infection thus allowing clearance of the infection, and concern of eventual expulsion, erosion, or exposure of matrix.
Related posts:
 49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
 47 Latissimus Dorsi Flap Anatomy
47 Latissimus Dorsi Flap Anatomy
 44 Two-Stage Prepectoral Prosthetic Breast Reconstruction
44 Two-Stage Prepectoral Prosthetic Breast Reconstruction
 42 Prepectoral Direct-to-Implant Breast Reconstruction
42 Prepectoral Direct-to-Implant Breast Reconstruction
 39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
 51 Transverse Rectus Abdominis Musculocutaneous Flaps
51 Transverse Rectus Abdominis Musculocutaneous Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


