38 Decision Making in Breast Reconstruction
Summary
Breast reconstruction confronts both the patient and surgeon with numerous options regarding subsequent reconstruction. This may include management of breast conservation deformity in the fall of longer plastic surgery or total mastectomy reconstruction. This chapter seeks to explore the decision-making processes involved in these two major avenues of reconstruction. The total mastectomy reconstruction discussion focuses on implant-based techniques with or without expanders, the latissimus flap with or without an implant and the fully autologous procedures incorporating donor sites from the abdomen, buttocks, and medial thighs. Included is a discussion on the dilemmas posed by radiation therapy and the timing of reconstruction in relation to it.
Key Teaching Points
Mastectomies will vary based on patient and oncologic factors and include nipple- and skin-sparing techniques that can be performed through a variety of incisions.
There are a variety of options for breast reconstruction following mastectomy that include prosthetic devices, autologous flaps, and oncoplastic techniques.
Proper patient selection is an important component when deciding on the optimal reconstructive option.
It is important to appreciate patient expectations and to set them appropriately prior to breast reconstruction.
Complications can occur following all forms of breast reconstruction and must be thoroughly explained and understood.
Novel strategies for breast reconstruction include prepectoral prosthetic reconstruction, perforator-based autologous flaps from a variety of donor sites, and oncoplastic surgery using augmentation and reduction mammaplasty techniques.
38.1 Introduction
When considering ablative breast surgery for cancer or prophylaxis, women are confronted with a variety of decisions. These range from the type of mastectomy (partial, total, skin-sparing, nipple–areolar sparing), to the type of reconstruction (prosthetic, autologous, oncoplastic), as well as the need for adjuvant therapy (chemotherapy, radiation). These decisions are complex and require significant research, thought, and counseling. The multidisciplinary approach in the management of breast cancer has facilitated the delivery of optimal care based on evidence and outcomes. This multidisciplinary team includes surgical, medical, radiation, and reconstructive oncology as well as the ancillary members that include nursing, geneticists, social workers, and other therapists.
The role of the plastic surgeon is to provide reconstructive options to women considering partial or total ablation of the breast. One of the caveats with breast reconstruction is that it does not interfere or impede with the oncologic aspects of breast care. This includes surveillance, delay of treatment, and adding physiologic stress. Oncologic considerations that may impact reconstruction include tumor size, tumor location, lymph node involvement, and metastatic cancer. Other relevant considerations are focused around the patient and include comorbidities, body characteristics, and expectations. The role of reconstructive surgery is now well appreciated and an integral component of the multidisciplinary care directed toward the well-being of the patient. This chapter will review many of the decision points that women cross when considering reconstructive surgery.
38.2 Indications for Breast Reconstruction
For many women, the breast represents a symbol of femininity, self-esteem, and self-image. The diagnosis of breast cancer can be a significant threat to all of these factors and the possibility of losing a breast can result in depression and withdrawal. The benefits of breast reconstruction are not only to restore the breast but also to enhance a woman’s self-esteem, identity, and body image. The journey that women are often confronted with is long and cumbersome and there are many decisions that need to be considered within a relatively short time. Decisions regarding breast reconstruction must be made early if considering immediate reconstruction following mastectomy; however, delayed reconstruction is also an option.
Perhaps the most important consideration is that the cancer be eradicated as completely as possible to reduce the risk of local recurrence and to ensure a tumor-free survival. The topic of breast reconstruction following total or partial mastectomy is usually mentioned following the initial diagnosis; however, a thorough discussion of breast reconstruction is provided once the patient has had the opportunity to process the diagnosis and its ramifications. Misconceptions regarding breast reconstruction are that it will delay treatment or that it will obscure the detection of a recurrence. Fortunately, studies have demonstrated that these are not true and have demonstrated the safety and efficacy of breast reconstruction following partial or total mastectomy.
For women having prophylactic mastectomy, the decision to proceed with breast reconstruction is less complicated and often a priority. For women with breast cancer, however, the decisions are complex because of the diversity of oncologic and reconstructive options and the importance of deciding which option is best for them. It is important for the multidisciplinary team to provide information regarding the types of mastectomies (skin-sparing vs. nipple-sparing), reconstructive options (prosthetic devices vs. autologous tissue vs. oncoplastic), adjuvant therapies (chemotherapy and radiation) as well as the important factors regarding recovery following surgery and reconstruction.
38.3 Total versus Partial Mastectomy
Current procedural statistics demonstrate that most women diagnosed with breast cancer will opt for breast conservation therapy (BCT) that involves lumpectomy and radiation. Small tumors are commonly treated in this fashion; whereas larger tumors are often treated with partial or total mastectomy. Reconstructive surgery is usually not necessary with BCT; however, it should be discussed with all patients considering partial or total mastectomy. Total mastectomy can be performed via skin-sparing mastectomy (SSM), nipple-sparing mastectomy (NSM), or areolar-sparing approaches. All are safe and effective in properly selected patients. NSM has become commonplace at many institutions, especially in the setting of prophylactic mastectomy. Although this technique is considered safe and effective, patient selection is important. Ideal candidates include those with small-to-moderate volume breasts, small tumors less than 3 cm, and tumors greater than 3 cm from the nipple–areolar complex (NAC); however, tumor size and distance from the NAC are becoming less relevant as long as an adequate margin is obtained. Women with large tumors near the NAC, moderate-to-severe mammary hypertrophy, or previous radiation may not be appropriate candidates for NSM but may be candidates for SSM. It is important for all women considering total or partial mastectomy to discuss these options with their plastic surgeon and breast surgeon.
38.4 Immediate versus Delayed Breast Reconstruction
Immediate breast reconstruction following mastectomy has become the most common option selected by the majority of patients choosing autologous or prosthetic reconstruction. Current procedural statistics estimate that over 50% of women will choose immediate reconstruction following partial or total mastectomy. The decision to proceed with immediate reconstruction is based on oncologic safety and reconstructive efficacy. Immediate reconstruction has been demonstrated to enhance body image, self-esteem, and quality of life and is considered in women with all stage I and II tumors and selectively offered to patients with stage III or IV tumors. Most women with inflammatory breast cancer are advised to forego immediate reconstruction due to the increased risk of local recurrence. Patients with metastatic disease are sometimes discouraged from immediate reconstruction in order to minimize the physiologic stress associated with breast reconstruction. In some situations, women with stage IV breast cancer can be considered for delayed reconstruction if tumor progression has stabilized; however, it is recommended that clearance from medical and surgical oncology be obtained prior to proceeding. Delayed reconstruction is sometimes recommended following mastectomy when the vascularity of the mastectomy skin flaps is compromised and at high risk for necrosis. In this situation, proceeding with immediate reconstruction may result in reconstructive failure if the mastectomy skin flaps do not survive. A safe alternative is the delayed immediate approach whereby the mastectomy skin flaps are closed without reconstruction followed by reconstruction 1 to 3 weeks later when tissue viability is confirmed. In some situations, delayed reconstruction may be recommended when adjuvant therapy including chemotherapy and radiation therapy is required. Delayed reconstruction can occur months to years following the initial mastectomy. Studies have demonstrated that complications following delayed reconstruction are fewer compared to the immediate setting.
38.5 Breast Reconstruction Options
Current statistics demonstrate that nearly two-thirds of women will have reconstruction following mastectomy. As previously stated, this can occur immediately following the mastectomy or on a delayed basis. Some women will opt not to have reconstruction because they are reluctant to have additional surgery, apprehensive about tumor recurrence, lack of plastic surgical availability, or have fears related to delaying treatment.
Reconstructive options can be divided into three types: prosthetic, autologous, and oncoplastic. Prosthetic reconstruction is regarded as a simpler operation with a shorter postoperative recovery. Autologous reconstruction on the other hand is a more complicated procedure with a longer recovery period. Oncoplastic breast reconstruction occurs at the time of partial mastectomy and before radiation therapy to minimize contour abnormalities. Women need to be aware of the risks and benefits of all of these options. Prosthetic reconstruction will not last forever and the implants will eventually require removal or replacement. Autologous reconstruction may be more complex; however, when successful (98–100% of the time), will last forever. Oncoplastic reconstruction results in high patient satisfaction but is always associated with postoperative radiation therapy. The decision as to which to choose will be based on oncologic factors as well as the patients’ anatomy and desires.
38.5.1 Prosthetic Reconstruction
Breast reconstruction using prosthetic devices is the most commonly utilized option in the United States and performed in nearly 80% of women following mastectomy. Prosthetic reconstruction can be performed in one or two stages. One-stage reconstruction is typically offered to women with a body mass index (BMI) less than 30, small-to-moderate breast volume, good-quality mastectomy skin flaps, and those having prophylactic mastectomy. Two-stage reconstruction is typically offered to women with thinner mastectomy skin flaps or with a skin deficiency that will require expansion prior to permanent implant placement. The majority of plastic surgeons prefer the two-stage technique because it provides another opportunity to optimize breast contour and position.
An important decision for women choosing prosthetic reconstruction is the nature of the devices. Current devices include tissue expanders and implants that are all made with an outer shell composed of a silicone elastomer and an inner compartment that is filled with either saline or silicone gel. Tissue expanders are usually inserted immediately at the time of mastectomy but can also be used on a delayed basis. They are partially filled with saline in the operating room. Following the operation, the tissue expander is sequentially filled in the clinic with saline through the integrated port until the desired volume is obtained. Following complete expansion, the tissue expanders are removed and exchanged for a permanent implant. These permanent implants will vary in terms of filler material (saline or silicone gel), surface (smooth or textured), and shape (round or anatomical). Most plastic surgeons will recommend and most women prefer silicone gel devices because they are soft and have a consistency that more closely resembles the natural breast. A few women, however, will express concern over the use of silicone gel devices based on the media reports from the early 1990s suggesting that they were not safe. Since then, hundreds of scientific studies have demonstrated that silicone gel implants are safe and effective and not associated with the development of connective tissue disorders, neuropathies, chronic fatigue, cancer, or other clinical disorders. As a result, the Institute of Medicine and the Food and Drug Administration (FDA) have declared them safe and effective and permissible for use in all women. It should be noted, however, that these devices will not last forever and that their life span is typically 10 to 15 years. Over time, local complications will become more likely to occur and include capsular contracture and rupture that will likely require removal or replacement.
The surface and shape characteristics of the implants are also important factors to consider. Surface characteristics include smooth or textured and shape characteristics include round or anatomical. Round devices can be textured or smooth whereas shaped devices are always textured. The texturing of shaped implants is important to promote adherence and prevent rotation. There are recent data to suggest that textured surface devices may result in less capsular contracture; however, some surgeons still prefer to use the smooth-surface devices because they may be associated with less rippling and wrinkling. Most patients who choose to have a shaped implant prefer silicone gel instead of saline. Physical characteristics of shaped implants include increased projection along the lower pole of the breast and improved contouring in the upper pole of the breast. Although these characteristics seem desirable, they are not necessary in all situations. It should be noted, however, that shaped devices are composed of a more highly cohesive silicone gel making them firmer to palpation than the round silicone gel devices. This increased cohesivity with shaped devices is necessary for them to retain their shape when implanted.
A recent concern regarding the use of textured surface implants is the formation of a cancer known as breast implant–associated anaplastic large cell lymphoma (BIA-ALCL). The incidence of BIA-ALCL has been estimated to occur in 1 patient per 30,000 at time of this chapter preparation. The association with textured surface breast implants is currently being studied and may be secondary to a prolonged inflammatory response to the surface. To date, there have been no cases of BIA-ALCL that are uniquely associated with the use of smooth-surface implants. During the initial consultation, patients considering textured surface devices should be informed of this risk and properly consented. Patients should be aware that the most common presentation is a fluid collection that usually occurs several years following the original insertion of the device. Early management includes total capsulectomy with or without implant exchange that usually results in complete cure.
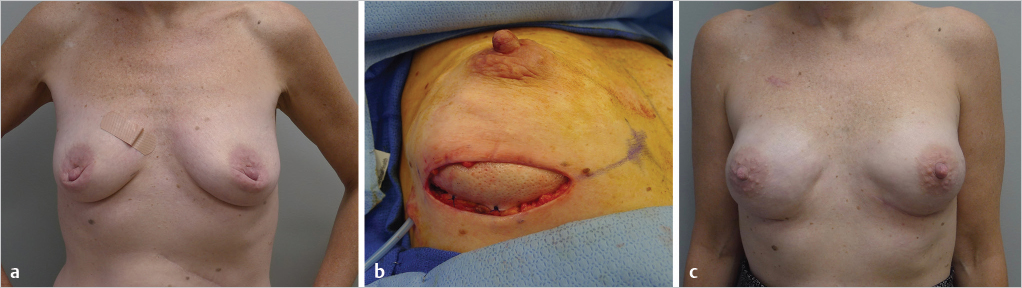
Another factor to consider with prosthetic reconstruction is where to place the implant or tissue expander. Devices can be placed partially or totally under the pectoralis major muscle or on top of the muscle. Current estimates are that the majority of plastic surgeons place breast implants partially or totally under the pectoralis muscle. When the device is placed partially under the muscle, it is important to stabilize the inferior edge of muscle to prevent upward migration known as “window-shading.” This can be achieved by stabilizing the cut inferior edge with sutures to the overlying skin or to use an acellular dermal matrix (ADM). The role of the ADM in this setting is to stabilize the position of the pectoralis major muscle, provide tissue support along the lower pole of the breast, provide an elastic environment, and to compartmentalize the prosthetic device on the chest wall. Limitations of total or partial muscle coverage techniques include pain or discomfort due to muscle spasm, a widened sternal cleavage plane because the medial origin of the pectoralis major does not usually correlate with the true medial border of the breast as well as implant malposition and animation deformity due to repetitive contraction of the pectoralis major muscle. ▶Fig. 38.1 illustrates a patient following NSM, two-stage reconstruction, partial muscle coverage, and use of ADM.
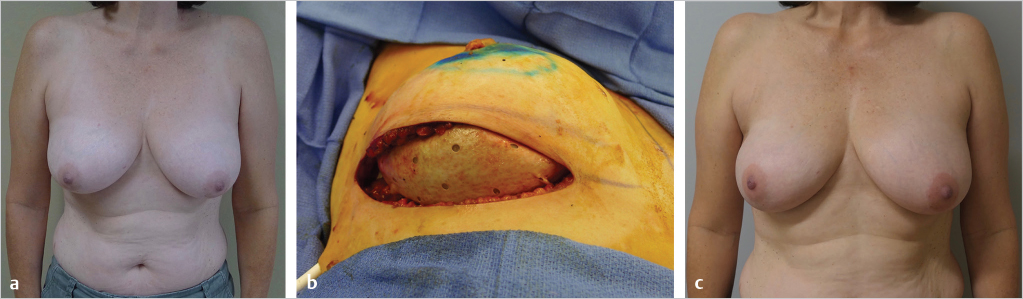
A recent innovation with prosthetic reconstruction is the prepectoral technique in which the breast implant or tissue expander is placed above the pectoralis major muscle. Advantages of the prepectoral position include no animation deformity, prosthetic placement that correlates with the natural breast, no muscle spasm, and easier recovery. Patients considering prosthetic reconstruction should be informed of the subpectoral and prepectoral options. The decision for prepectoral reconstruction is usually made in the operating room following the mastectomy and dependent on the quality and the vascularity of the mastectomy skin flaps. Prepectoral placement of breast implants should not be considered when the skin flaps are poorly perfused or there is visible dermis. ▶Fig. 38.2 illustrates a patient following two-stage reconstruction, prepectoral placement of the implant, and use of ADM.
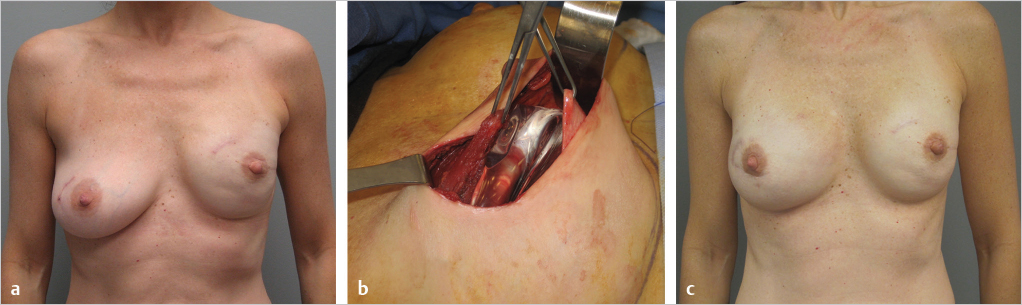
From a patient’s perspective, the one-stage or direct-to-implant operation may seem more desirable than a two-stage operation; however, there are factors that preclude this from being performed routinely. Direct-to-implant reconstruction is frequently considered in women with healthy and robust mastectomy skin flaps whereby the device can be placed prepectorally or subpectorally. This is especially considered in women having prophylactic mastectomy where the mastectomy skin flaps are usually more conducive toward this option. Patients having therapeutic mastectomy will often have thinner mastectomy skin flaps that may not be able to tolerate placement of a prefilled breast implant. Although one-stage reconstruction is an excellent option, the majority of plastic surgeons prefer two-stage prosthetic reconstruction because it provides for optimal implant selection, modification of the pocket, and optimal compartmentalization. Thus, in properly selected patients, both one- and two-stage reconstruction can provide excellent outcomes that are predictable and reproducible. ▶Fig. 38.3 illustrates a patient following one-stage prosthetic reconstruction.
Monitoring and surveillance of women with breast implants following mastectomy is important. Because the breast parenchyma has been removed, mammography is not usually necessary. Magnetic resonance imaging or ultrasound is typically recommended when there are palpable abnormalities, oncologic concerns, or to assess the integrity of the implants. For women with silicone gel breast implants, the FDA has recommended that imaging be performed at 3-year intervals to assess the integrity of the implant to rule out silent rupture of the device. Because breast implants are typically made with a highly cohesive silicone gel, rupture is not usually associated with gel migration. Instead, the silicone gel usually remains within the fibrous capsule of the implant. In the event of a rupture, device exchange or removal is usually recommended.
Pearls
Prosthetic reconstruction accounts for approximately 80% of all breast reconstruction procedures in the United States.
Two-stage reconstruction with tissue expanders followed by permanent implants is considered to be more predictable and reproducible.
Acellular dermal matrices provide tissue support, implant compartmentalization, an elastic space, and may minimize the incidence of capsular contracture.
Women with prosthetic devices are encouraged to have surveillance every few years to assess for silent rupture.
Prepectoral placement of devices eliminates animation deformity and muscle spasm.
Prosthetic reconstruction can result in capsular contracture, displacement, rupture, and premature removal.
Related posts:
 49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
49 Preventing and Managing Complications in Latissimus Dorsi Flap Reconstruction
 47 Latissimus Dorsi Flap Anatomy
47 Latissimus Dorsi Flap Anatomy
 44 Two-Stage Prepectoral Prosthetic Breast Reconstruction
44 Two-Stage Prepectoral Prosthetic Breast Reconstruction
 42 Prepectoral Direct-to-Implant Breast Reconstruction
42 Prepectoral Direct-to-Implant Breast Reconstruction
 39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
39 Prepectoral Breast Reconstruction: Direct-to-Implant versus Two-Stage
 51 Transverse Rectus Abdominis Musculocutaneous Flaps
51 Transverse Rectus Abdominis Musculocutaneous Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


