30 Breast Surgery after Massive Weight Loss
Summary
This chapter covers key concepts and an effective surgical approach for severe changes in breast shape associated with massive weight loss. The nature of the deformities, including profound deflation of the skin envelope and a lateral roll of skin and fat with descent of the lateral inframammary fold, is described. For patients with adequate breast volume, a dermal suspension mastopexy with parenchymal reshaping and selective autoaugmentation can be performed. This procedure provides multiple points of fixation to the chest wall and enables reshaping of the breast for enhanced lateral curvature, projection, and elimination of the lateral roll of skin and fat. Other approaches to breast reshaping are also described.
Key Topics
Anatomical considerations.
Severity of deformity and recommended technique.
Indications for dermal suspension/parenchymal reshaping with selective autoaugmentation.
Choice of technique:
Patients with excessive breast volume.
Patients with inadequate breast volume.
Patients with adequate breast volume with significant ptosis and skin redundancy.
Operative technique.
Combined procedures.
Key Teaching Points
Maintaining a thickness of at least 1 to 1.5 cm on the skin flaps improves contour and minimizes tissue loss at the inverted-T point.
The surgeon should not leave the operating room until happy with the dermal plication and the appearance of the breast shape and projection after the skin flaps are redraped. Shaping of the breast is performed in real time to the satisfaction of the surgeon.
The nipple–areola complex is occasionally tethered by the dermis, which can be partially released around its circumference to allow it to be easily transposed to the keyhole pattern without tension.
When combining breast surgery after massive weight loss with abdominal contouring, the abdominal procedure should be done first.
Observations
Obesity continues to rise in the United States at an alarming rate, with more than 35% of Americans considered obese. To lower their risk of obesity-related medical conditions, many people have sought to lose weight through either bariatric surgical procedures or diet and exercise. After massive weight loss, defined as the loss of more than 50 pounds, patients are often left with redundant skin and excess subcutaneous tissue. For this reason, an increasing number of patients are consulting plastic surgeons for correction of these deformities. The abdomen is the most frequent area of concern, but many women are troubled by the appearance of their breasts after massive weight loss. Most of these women had full breasts before their weight loss and have severe deformities after reaching their goal weight. This chapter highlights the anatomical changes observed in the breast after weight loss and presents details of a versatile technique to achieve an aesthetically pleasing result.
30.1 Anatomical Considerations
Women who have undergone massive weight loss have characteristic breast deformities that distinguish them from other women who seek correction of volume loss and breast ptosis. The Pittsburgh Rating Scale describes the spectrum of deformities seen after massive weight loss, with most patients exhibiting the more severe grades. This scale was designed to classify postbariatric deformities; it was developed in recognition that the standard ptosis grading scale was not descriptive enough to characterize the unique changes in breast shape inherent in this population.
The least severe deformities involve grade 1 or 2 ptosis, or macromastia. The midrange deformities (Pittsburgh Scale Severity 2 out of 3) demonstrate grade 3 ptosis and can still be treated with traditional breast reshaping techniques. The most severe deformities (Pittsburgh Scale Severity of 3 out of 3) have one or both of the findings unique to massive weight loss patients: severe volume depletion with a flattened breast shape and/or a prominent lateral roll of skin and fat that merges the breast mound with the upper back tissues. Additionally, in any patient who has undergone massive weight loss, the nipples may be medialized. Failure to recognize this finding and move the nipples laterally along a true breast meridian is a pitfall of breast reshaping in massive weight loss patients (▶Table 30.1).
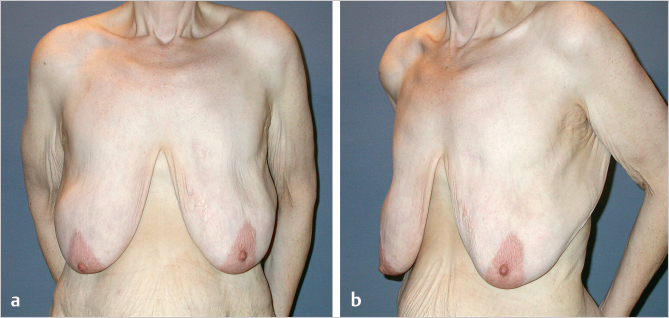
The changes in breast shape after weight loss, in the most severe form, are characterized by two findings that pose significant technical challenges. The first finding is volume loss with a stretched skin envelope and flattening of the breast against the chest wall (▶Fig. 30.1).
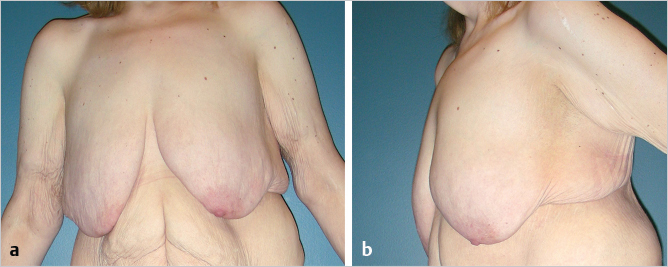
The second finding is a roll of skin and fat on the lateral border of the breast that extends onto the chest wall. This roll of skin and fat obscures the lateral curve of the breast, an important aesthetic unit. The technique of dermal suspension and selective autoaugmentation described in this chapter can correct these deformities and restore breast shape by using available parenchyma to build projection and recruiting the lateral chest wall tissue into the breast mound. In any massive weight loss patient, one must also be aware that the nipple position may be abnormally medial and should be repositioned along a true breast meridian (▶Fig. 30.2).
30.2 Patient Evaluation
30.2.1 History
When evaluating any massive weight loss patient, the surgeon should take a detailed history, including the type of weight loss surgery, time elapsed since the weight loss surgery, the patient’s initial body mass index (BMI), and current BMI. The patient should be as close to goal weight as possible (a BMI under 30 is preferable) and at a stable weight (no more than a 2.3-kg [5-pound] change per month) for 3 months. This weight stabilization often occurs 12 to 18 months after a gastric bypass procedure. For patients with a BMI over 35, the surgeon should consider referring the patient back to the weight loss specialists to provide diet and exercise programs to optimize the patient’s BMI before surgery.
30.2.2 Physical Examination
Physical examination of the breast should include a careful search for masses. Parenchymal volume should be assessed, along with the presence and size of a lateral roll of skin and fat. The surgeon should determine whether the native breast parenchyma and lateral roll together will provide adequate volume for a breast reshaping procedure. Prior scars should be noted and considered regarding their impact on blood supply for the procedure selected. Mammography is performed in accordance with the American Cancer Society guidelines.
30.3 Indications for Dermal Suspension/Parenchymal Reshaping with Selective Autoaugmentation
Severe ptosis with a deflated breast shape.
Adequate parenchymal volume to build a breast mound, including consideration of lateral chest wall tissue volume that can be recruited.
Lateral skin roll (not required to perform this procedure, but allows recruitment of chest wall tissue into the breast mound).
30.4 Contraindications to Dermal Suspension/Parenchymal Reshaping with Selective Autoaugmentation
Absolute contraindication:
Active tobacco user.
Relative contraindications (proceed if safety not compromised):
Inadequate parenchymal volume to build breast mound (relative contraindication because lateral roll volume needs to be considered and may add sufficient volume).
Prior scars on breast.
Active intertrigo.
BMI over 35.
There are relatively few contraindications to the procedures mentioned above. Patients who are current users of tobacco products are instructed to stop for 1 month before and after surgery. We routinely screen patients with a positive history of smoking with a cotinine urine test before surgery. Patients who have had previous breast surgery must be carefully evaluated to ensure that their old scars will not compromise any planned procedure. Patients with active intertrigo or diffuse fibrocystic disease may also not be ideal candidates.
30.5 Operative Planning
30.5.1 Choice of Technique
Many procedures have been described to correct the breast deformities seen in massive weight loss patients. The severity of each of the previously described deformities, the preferred breast size of the patient, and the surgeon’s experience will all influence the type of procedure offered. Each patient is unique, and the procedure chosen must not only address each aspect of the breast deformity, but it must also be able to produce the size and shape that the patient desires.
Excessive Breast Volume: Pittsburgh Scale Grade 1
Even after massive weight loss, some patients maintain significant breast volume despite varying degrees of ptosis. Women who want their breasts to be smaller than their current size will require a breast reduction procedure. Although short-scar techniques have increased in popularity, the skin redundancy and poor skin elasticity in such patients will result in a large inferior dog-ear that will require horizontal excision. The pitfall of the short-scar techniques in these patients would be the need to chase the dog-ear inferiorly, leaving an unsightly scar below the inframammary fold (IMF).
A predictable shape and size can be achieved using a Wise pattern skin excision. This excision will often need to be carried out laterally onto the breast to excise redundancy in this area. A medial or inferior pedicle can be used, depending on the nipple to inframammary fold distance and the experience of the surgeon.
Because of the medial positioning of the nipple in many patients who have undergone massive weight loss, it may be difficult to get adequate nipple rotation if a medial pedicle is chosen. This must be given consideration in the preoperative planning. Liposuction of the lateral fold can also be a useful adjunctive procedure to assist in contouring the lateral region of the breast.
Related posts:
 22 Periareolar Mastopexy
22 Periareolar Mastopexy
 16 Subfascial Inframammary Breast Augmentation
16 Subfascial Inframammary Breast Augmentation
 31 Vertical Superior Pedicle Breast Reduction (Modified Lassus Technique)
31 Vertical Superior Pedicle Breast Reduction (Modified Lassus Technique)
 42 Prepectoral Direct-to-Implant Breast Reconstruction
42 Prepectoral Direct-to-Implant Breast Reconstruction
 54 Prevention and Management of Complications in DIEP Flap Reconstruction
54 Prevention and Management of Complications in DIEP Flap Reconstruction
 9 Fat Grafting to the Breast: Aesthetic and Reconstructive Applications
9 Fat Grafting to the Breast: Aesthetic and Reconstructive Applications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


