31 Vertical Superior Pedicle Breast Reduction (Modified Lassus Technique)
Summary
Vertical short-scar breast reduction is a technique designed to reduce the breast while minimizing breast scarring, preserving upper pole fullness, reducing the transverse diameter of the breast, and enhancing breast shape. The procedure utilizes a superior pedicle.
Central pyramidal excision and medial and lateral inframammary wedge resections are combined to shape the breast. The chapter also discusses the liposuction of the tail of the breast.
Key Teaching Points
Perform liposuction only on the tail of the breast.
Thin the pedicle progressively from the base toward its tip leaving a broad base for optimal blood supply.
Always perform inframammary wedge resections to reduce the risk of a boxy breast and to shape the inframammary fold.
Create equal vertical pillar lengths medially and laterally.
Always drain these reductions.
Modify the markings to incorporate a larger areolar diameter for larger-breasted more ptotic women in order to reduce vertical limb length.
31.1 Introduction
The French plastic surgeon, Claude Lassus, pioneered the superior pedicle vertical breast reduction. Madeleine Lejour from Belgium became a major proponent of the procedure, and added liposuction of the entire breast as well as a pedicle suspensory suture to the chest wall to maintain upper pole fullness. She later noted increased fat necrosis with total breast liposuction. She abandoned this component of the technique in favor of liposuction of the tail of the breast only, in an effort to decrease the transverse diameter of the breast as well as defining the lateral breast crease. Variations of these two procedures form the basis of this chapter. While retaining liposuction of the tail of the breast, I have completely abandoned the suspensory suture in the superior pedicle as it appeared to distort the shape of the breast.
Key Advantages of the Procedure
Narrows the transverse diameter of the breasts.
Removes fat from the lateral breast and chest wall to create a well-defined lateral breast crease.
Removes ptotic tissue through inframammary and central lower breast resections.
Avoids the undesirable medial and lateral inframammary incisions by using a vertical closure.
Elevates the inframammary crease where necessary.
Maintains fullness in the upper and medial quadrant of the breast where it is most needed.
Breast width is reduced transversely and shortened vertically, by using this technique. It decreases the base diameter of the breast and can elevate the inframammary crease if desired. A significant volume of breast parenchyma can be removed through excision of the lower breast parenchyma where glandular ptosis is often most troubling, and the inframammary fold (IMF) elevation decreases the amount of skin traditionally resected, resulting in shorter vertical scars. Elevation of the IMF converts lower breast skin to chest wall skin and makes the breasts appear elevated and more youthful.
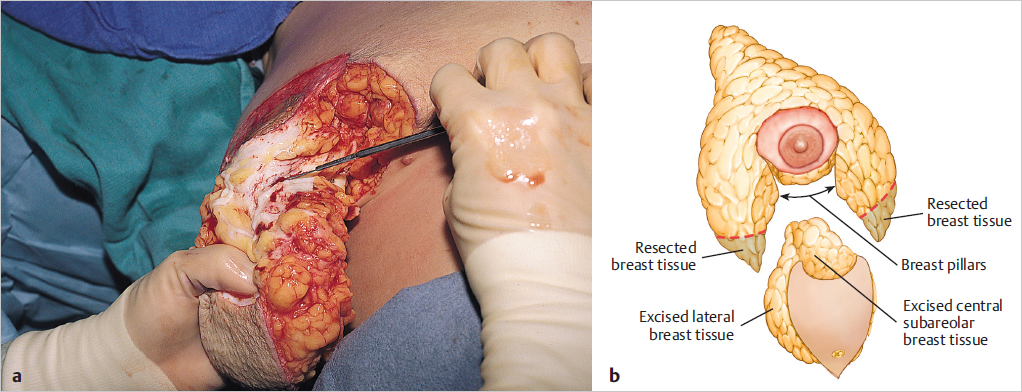
The basic operative concept is illustrated diagrammatically in ▶Fig. 31.1.
Surgical Plan
Preoperative marking—nipple–areolar complex (NAC), vertical pillars.
Tumescent infiltration, liposuction tail of breast.
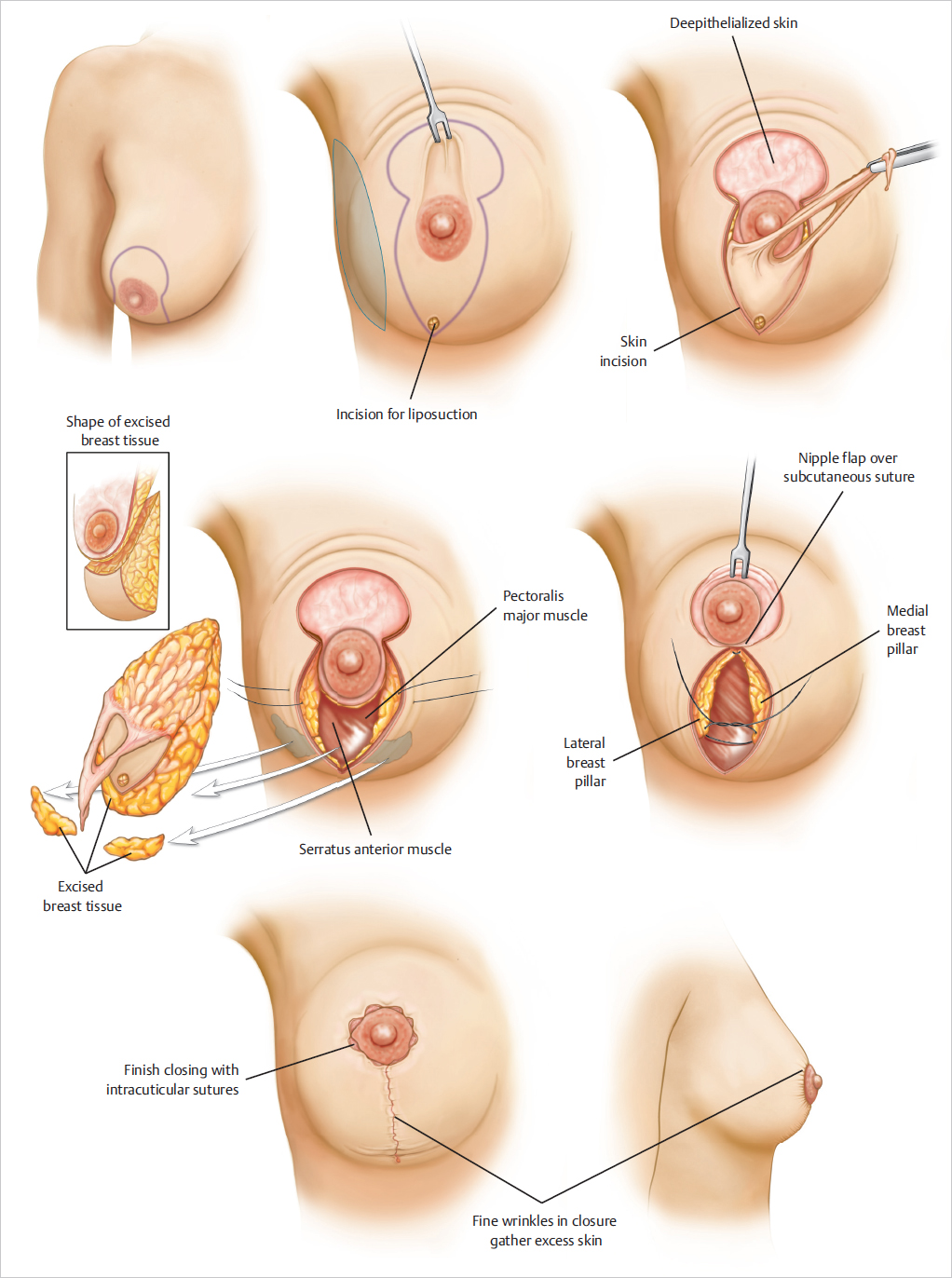
Incise nipple–areola circumference and deepithelialize superior pedicle.
Resect central pyramid and create medial and lateral pillars. Resect medial and lateral wedges at inframammary fold.
Approximate medial and lateral pillars, insert drain.
Inset NAC.
Apply dressings.
31.2 Technique
31.2.1 Markings Nipple-Areolar Complex
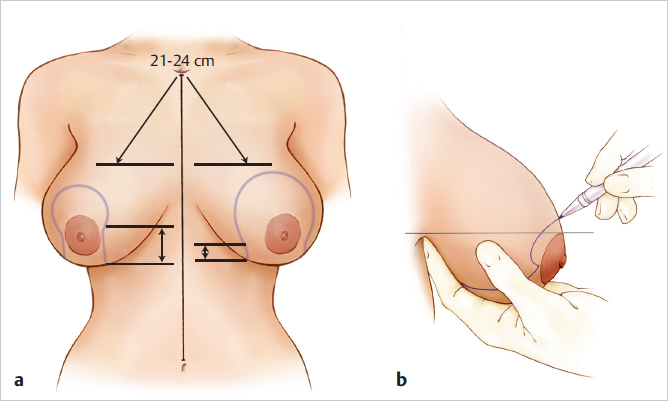
The patient is marked preoperatively in the erect position. The top of the future areola is marked; it should be located about 2 cm above the inframammary fold. I usually place it 1 cm lower than I would for a standard Wise pattern reduction, typically at a 22- to 23-cm nipple-to-notch measurement, allowing for superior drift of the areola once the inferior weight of the breast has been resected. A large, C-shaped dome incision is made with its open side inferior. The larger the breast, the larger the C-shaped dome. Typically, a smaller breast has a C circumference of around 12 to 13 cm. A large-breasted woman may have a circumference of 19 to 21 cm. At the close of the procedure, this C shape has to be closed around a recipient areolar diameter of 38 to 42 cm (▶Fig. 31.2).
Vertical Limb Marking
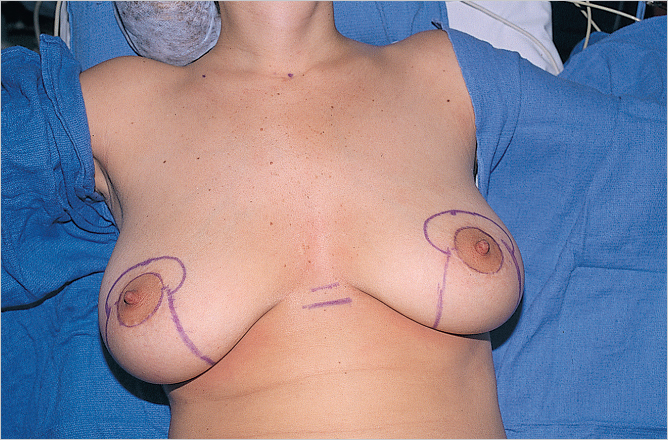
The vertical limbs of the breast incision are marked next by displacing the breast medially and laterally, dropping perpendiculars at the level of the meridian of the breast. Starting from the base of the medial inferior limits of the C-dome marking, a perpendicular line is dropped down toward a point approximately 3 cm above the IMF with the breast pushed laterally by the left hand. Next, the lateral vertical line is marked. This is achieved by displacing the breast medially and dropping a perpendicular from the inferior most limits of the lateral portion of the C dome down to about 3 cm above the IMF (▶Fig. 31.3).
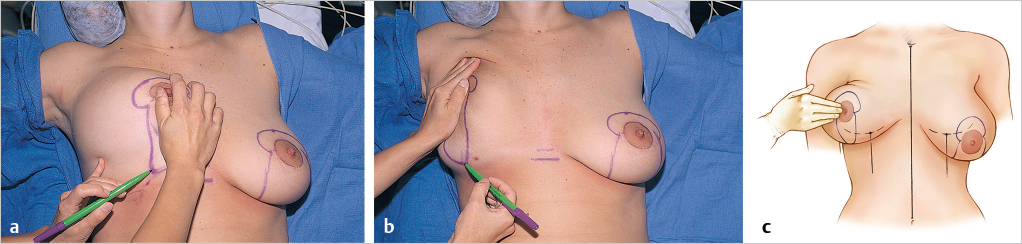
This creates two vertical limbs fanning out medially and laterally from the C-dome shape without being connected inferiorly. The breast is then displayed superiorly, which pulls the two vertical limbs into a more vertical orientation, and they can then be joined by a gentle U shape, 1 or 2 cm above the inframammary crease (▶Fig. 31.4).
Clinical Pearl
It is important to create the U-shaped connecting lines above the inframammary crease in order to prevent migration of the scar down onto the chest wall below the breast and below the bra strap line.
The amount of force placed on the displaced tissue will be reflected in the corresponding tightness of the closure. The displacement should not be so firm if more skin is required for the closure. The position of the upper areola is marked, and an ellipse the width of the areola is drawn upward to connect the medial and lateral lines.
31.2.2 Operative Positioning
The patient is prepped and draped on the operating table. Her arms are abducted and secured to arm boards so that she can be elevated to an upright position during the operation to confirm symmetry.
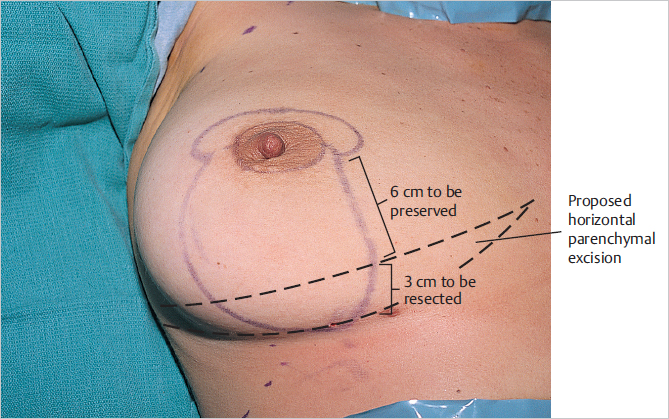
The vertical extent of the breast parenchyma to be preserved is determined. This is usually 5 to 6 cm below the future areolar site. This point is marked, and if necessary, an ellipse is drawn below this point toward the IMF to delineate the amount of transverse parenchymal resection (▶Fig. 31.5).
31.2.3 Tumescent Infusion and Liposuction
A single stab wound is made with a No. 15 blade into the base of the breast at the apex of the U incision connecting the two vertical limbs. Wetting solution is infiltrated laterally into the tail of the breast to facilitate liposuction of this area. Additional wetting solution is also infiltrated into the breast parenchyma along the vertical resection lines and inferior central breast to be resected in order to reduce intraoperative bleeding. A standard tumescence cannula and infusion pump is used (▶Fig. 31.6).
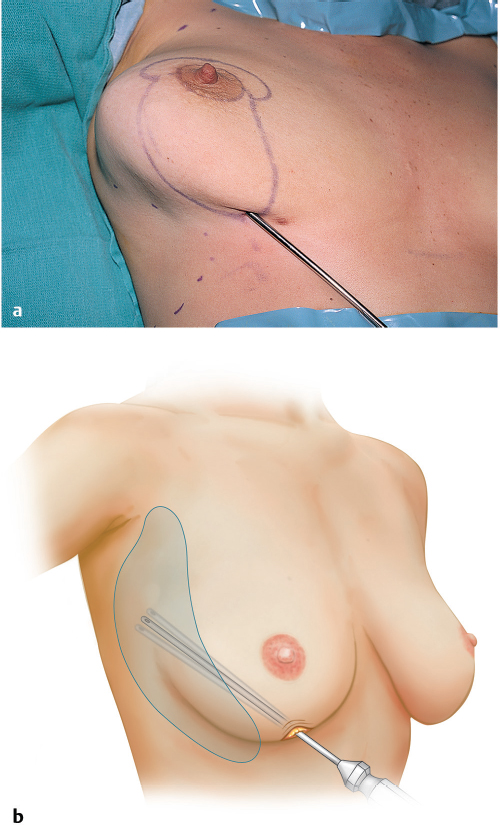
31.2.4 Liposuction in Vertical Mammaplasty
Power-assisted liposuction with a 5-mm cannula is used for lateral breast suction. This helps define the lateral breast crease and narrows the breast, as well as reducing circumferential chest circumference to some extent.
Liposuction is limited to the axillary tail and lateral breast, so as not to compromise blood flow to the superior pedicle. After liposuction, the lateral chest and breast may be bruised for 1 to 2 weeks and remain tender, swollen, and firm for several weeks. Most women note that there is more pain and discomfort in the areas of liposuction than in the breast reduction itself.
This technique requires an artistic eye to shape the lateral breast crease and chest wall appropriately. Resection volumes range on average from 100 to 300 mL per side, but heavier women may yield up to 1 L of liposuction volume per side in rare cases. Care should be taken to maintain the balance between tumescent fluid infusion and resection volumes.
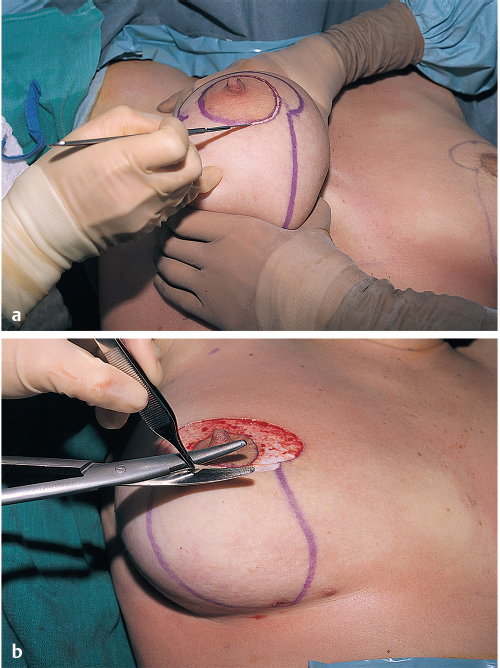
31.2.5 Incise Areola and Deepithelialization of Superior Pedicle
The operative procedure is begun by incising the areolar diameter, the periareolar inset, and the outline of the superior pedicle. The superior pedicle is deepithelialized with either a No. 20 blade or curved Mayo scissors. This maintains the subdermal plexus in order to preserve areolar blood supply (▶Fig. 31.7).
31.2.6 Pillar Dissection
Cutting the pillars can be divided into the following three components:
Cutting and shaping the medial pillar.
Cutting and shaping the lateral pillar.
Connecting the two pillars with a U-shaped incision above the IMF.
Medial Pillar Dissection
With the breast displaced laterally, the medial breast parenchyma is incised vertically from the lower areolar marking downward to the point of the U. The cut edge of the medial pillar should be 2-cm thick, tapering thicker medially as the dissection proceeds toward the level of the prepectoral fascia on the chest wall. This provides a progressively thicker medial flap as it is carried down toward its base, preserving medial perforators for perfusion. It also provides medial fullness to enhance cleavage formation (▶Fig. 31.8).
Lateral Pillar Dissection
The breast is displaced medially and the lateral limb is incised vertically toward the chest wall for a thickness of 2 cm. This is then beveled laterally following the curve of the chest wall, creating a progressively thicker flap toward its base. Care should be taken not to leave too much lateral bulk toward the base of the flap as this will contribute to excessive lateral fullness in the final result. This dissection should be carried down to the fascia overlying serratus anterior (▶Fig. 31.9).
31.2.7 Connecting the Vertical Limbs
With the medial and lateral limbs shaped, the base of both incisions is connected with a U-shaped incision the base of which should be at least 2 cm above the preexisting inframammary crease. It is imperative when dissecting the breast tissue of this U-shaped incision that the plane of dissection be immediately subdermal. No fat should be left on the skin at this point so as to limit dog-ear formation postoperatively. Dissection should be carried down to the pectoralis fascia (▶Fig. 31.10).
Technical Pearl
The breast tissue between these two incision lines defines the lower pole breast parenchymal resection.
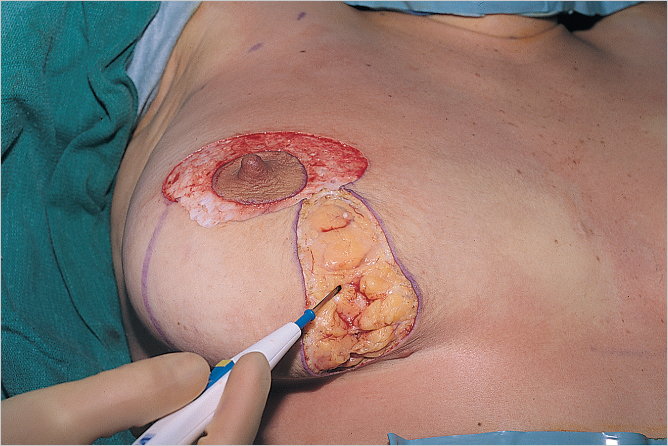
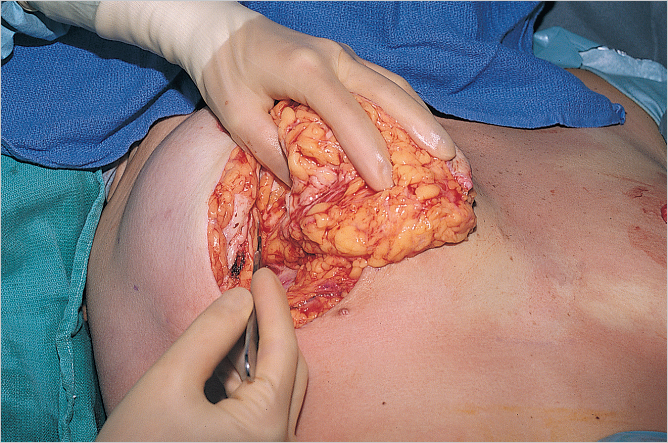
31.2.8 Central Pyramidal Breast Flap Elevation
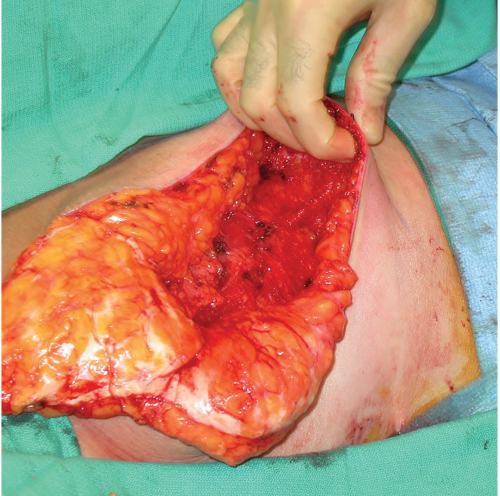
With the medial and lateral and inferior boundaries of the central breast resection defined, the flap can now be dissected of the underlying pectoralis major muscle in preparation for excision. The inferior base of the flap just above the IMF is grasped with an Allis tissue forceps and is dissected off the pectoralis major with electrocautery, controlling perforators as they are encountered. Dissection is carried in a cephalad direction to a point level with an imaginary transverse line drawn between the two lowermost tips of the inverted C dome drawn for the nipple–areola inset (▶Fig. 31.11).
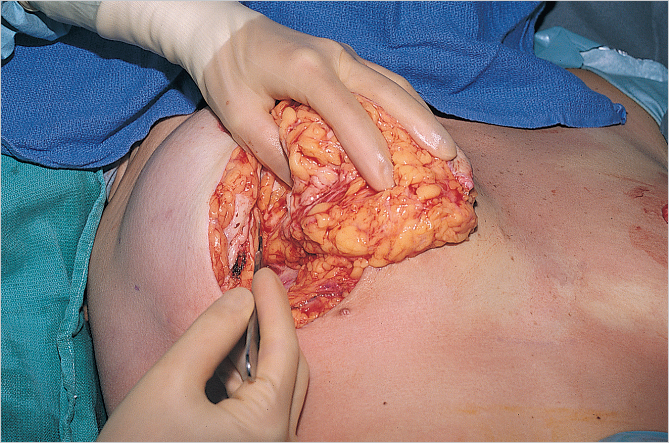
31.2.9 Shaping the Superior Pedicle
Starting just below the areola, a vertical incision is made to a depth of 1 to 2 cm. The angle of dissection is then turned underneath the areola in a cephalad direction heading toward the base of the breast on the pectoralis major muscle in the upper pole. This creates a beveled pedicle starting 1- to 2-cm thick at its tip then thickening toward the base of the pedicle on the chest wall (▶Fig. 31.12).
This performs two functions:
It maintains upper pole fullness in the long term.
It captures perforators from the thoracoacromial axis as well as the second and third internal mammary perforators to preserve nipple–areolar blood supply.
The central parenchymal resection is allowed to fall away from the pedicle as it is shaped and is removed (▶Fig. 31.13).
By lifting the breast off the lower deep fascia, the surgeon can assess the medial and lateral pillars of the breast. If additional breast tissue requires resection, deep lateral tissue is usually removed to reduce lateral breast volume and fullness.
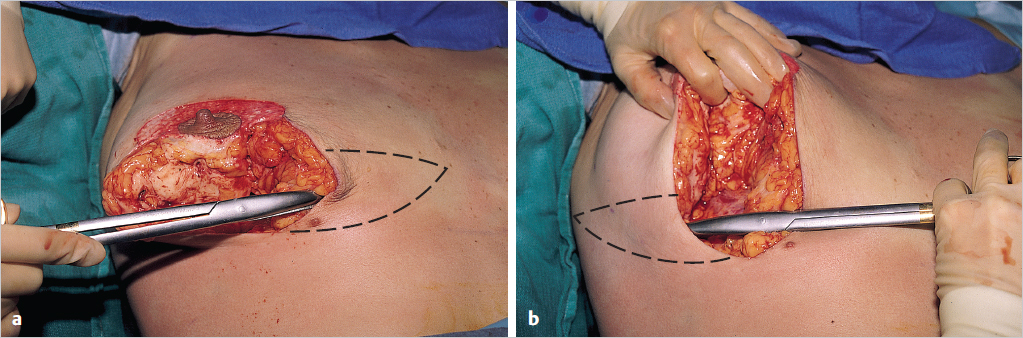
31.2.10 Medial and Lateral Inframammary Wedge Resection
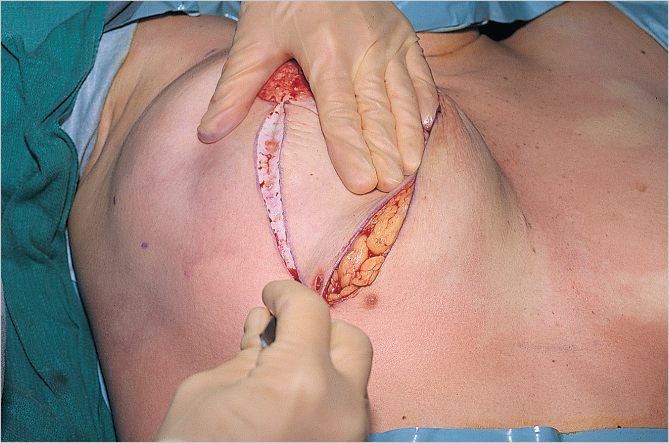
The lower breast skin just above the IMF is undermined at the immediate subdermal level in preparation for removal of the medial and lower lateral breast parenchyma. If this is not done, excessive breast tissue will be left on the skin flaps, which prevents the inevitable dog-ear at the base of the breast from collapsing fully into the adjacent dead space (▶Fig. 31.14).
The lower 3 to 4 cm of breast skin is undermined medially and laterally. With the central resection completed, medial and lateral inframammary wedge resections are performed. These are carried out from the pectoralis major fascia up to the dermis. No tissue should be left behind, in an effort to minimize dog-ear formation. The width of the wedges is based on the planned vertical length of the edges of the medial and lateral pillars; this provides the proper proportions for the reduced breast (▶Fig. 31.15).
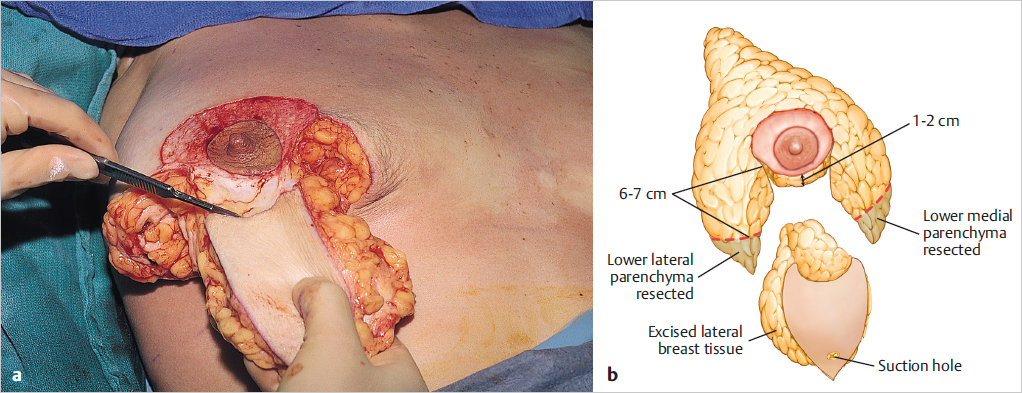
The medial, lateral, and central resections are shown. Most of the resection is performed centrally in the lower breast, the location of the breast parenchyma that is responsible for most ptosis (▶Fig. 31.16).
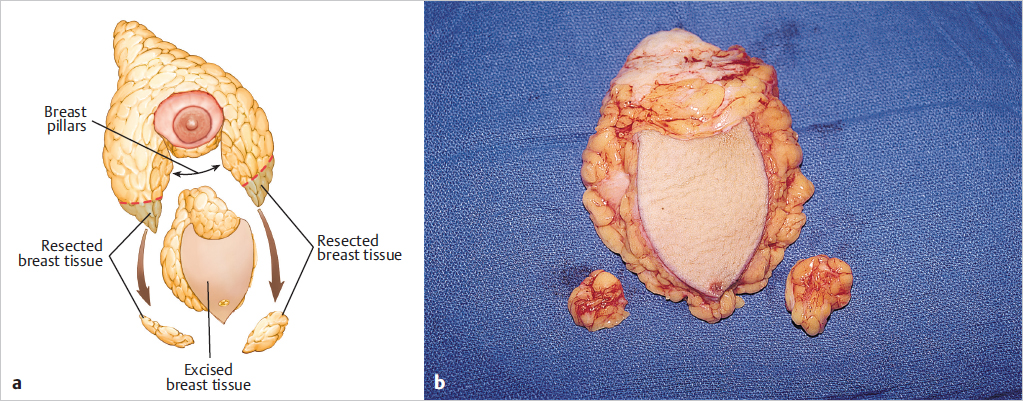
The central resection leaves a superior pedicle, as shown in ▶Fig. 31.17. The pedicle tip is 1- to 2-cm thick, beveling thicker toward its base to preserve blood supply.
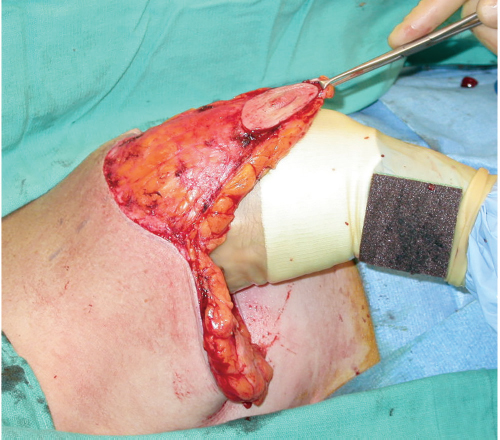
Technical Pearl
A common mistake during the learning curve with this operation is to leave the pedicle too thick, which limits its ability to fold easily and creates venous engorgement that, in turn, can lead to nipple congestion and loss.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


