Abstract
This chapter examines the anatomy, pathology, and treatment of Dupuytren’s disease and the not uncommon malady known as trigger finger. Surgery is typically the only remedy for Dupuytren’s, and the authors guide the reader through the intervention options. Trigger finger presents as a catching or locking sensation in the digits, and treatment—nonsurgical or surgical—depends on the severity of the problem. For the surgical option, the authors describe each step of the procedure and caution about possible complications. Postoperative dressings are reviewed and expected outcomes cited at the conclusion of the chapter.
29 Dupuytren’s and Trigger Finger
29.1 Dupuytren’s Disease (Palmar Fibromatosis)
29.1.1 Goals and Objectives
To understand the anatomy and pathology of at-risk patient populations for Dupuytren’s disease.
To understand the surgical indications and options for Dupuytren’s patients.
To be able to avoid potential complications of Dupuytren’s surgery and educate patients appropriately on expectations of surgery and the risk of recurrence.
29.1.2 Patient Presentation
A typical presentation of a patient with Dupuytren’s disease is described: A 60-year-old man of Scandinavian descent presents with progressive flexion contracture of his ring and little fingers over the last 6 months. The deformity is causing inability to perform daily tasks with his right hand which originally began with a painful nodule in his palm. This became non-painful over time despite developing into a larger cord of tissue. His father had a similar condition in the past. On physical exam, he has a metacarpophalangeal (MCP) joint flexion contracture of 45 degrees and a proximal interphalangeal (PIP) joint contracture of 45 degrees along with palpable cords to both the ring and little fingers. He has normal sensation and vascular flow to the fingers. Radiographs show no arthritis of the hand and no other anomalies.
29.1.3 Preparation for Surgery
Dupuytren’s disease is a disease more predominant to males over the age of 40 years and of Northern European descent, traditionally Scandinavian region and the regions in which Viking conquests took place. 1 It is a proliferation of collagen with an increase in ratio of Type III to Type I collagen in the palmar fascia creating pathologic cords from the normal bands. Myofibroblasts and fibroblasts are the implicated cell lines with residual myofibroblasts in adjacent dermal and epidermal tissues being thought to contribute to recurrence. 1 , 2 , 3 Typically, Dupuytren’s disease is diagnosed by history and physical exam alone with plain radiographs used to evaluate for any concomitant osteoarthritic changes of contracted joints. MRI and CT evaluations are typically unnecessary. Biopsy is also typically unnecessary unless the presentation is atypical and there is a concern for malignant mass; however, this is a rare presentation.
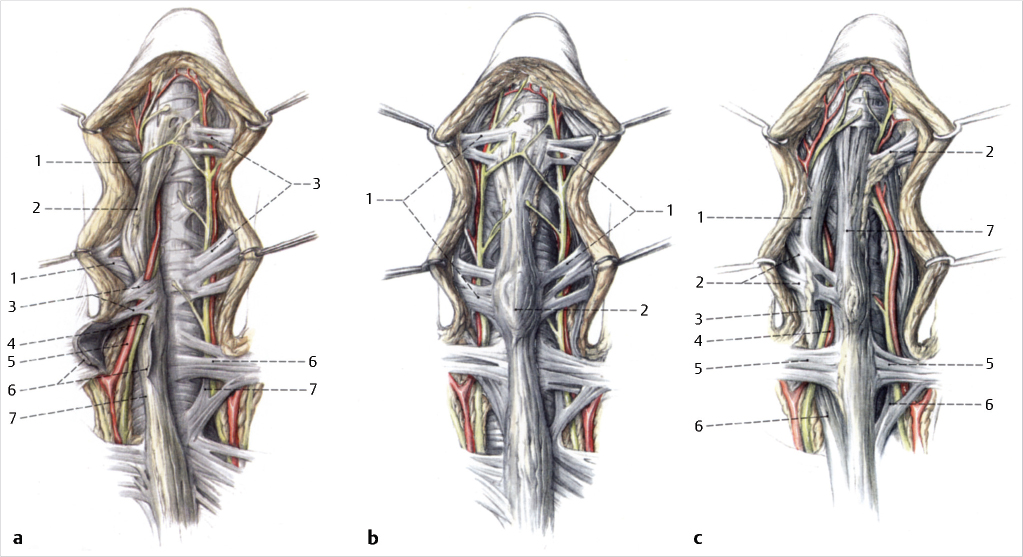
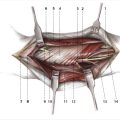
Understanding of the pathoanatomy is critical in Dupuytren’s disease (Fig. 29‑1). Normally, as the palmar fascia travels distally toward the digits, it becomes pretendinous bands (Fig. 29‑2). The portion that bifurcates to each digit then becomes spiral bands and traverses to the lateral sheets in the ulnar and radial aspect of each digit which also coalesce and connect to the coronally oriented perineurovascular fascial sheets named “Cleland’s and Grayson’s ligaments” which attach to the flexor apparatus centrally and the dermis peripherally. Grayson’s ligament is volar to the neurovascular bundle and can be involved in Dupuytren’s disease, while Cleland’s ligament is dorsal and not involved in the disease process. In the distal palm and toward the digits, the spiral bands become dorsal and more peripheral than the neurovascular bundle. In the diseased hand, the bands become pathologic cords and thicken to become spiral cords. The neurovascular bundles are then displaced centrally and more superficial. These changes lead to cutaneous pitting, MCP joint flexion contracture, and, sometimes, PIP joint contracture as well (Fig. 29‑2; Fig. 29‑3).

29.2 Treatment
Dupuytren’s disease does not predictably resolve or improve with nonoperative treatments such as splinting, ointments, creams, or therapy. 4 Patient education is important for self-monitoring for progression of deformity as it can be slowly progressive and painless. The “table top” test whereby a patient attempts placement of his/her palm flush on a table is helpful. Inability to perform this task can be associated with MCP joint contracture of 30 to 40 degrees. 4 Intervention is standardly recommended for MCP joint contracture of 40 degrees or more in one digit, and if treating that digit, then contracture of other digits may be considered even if deformity is only 20 to 30 degrees. PIP joint contracture is more difficult to improve and some authors advocate for intervention in cases of any contracture; however, McFarlane recommends intervention only when it is more than 30 degrees due to potential risk of actually worsening the disease for interventions at lower degrees.
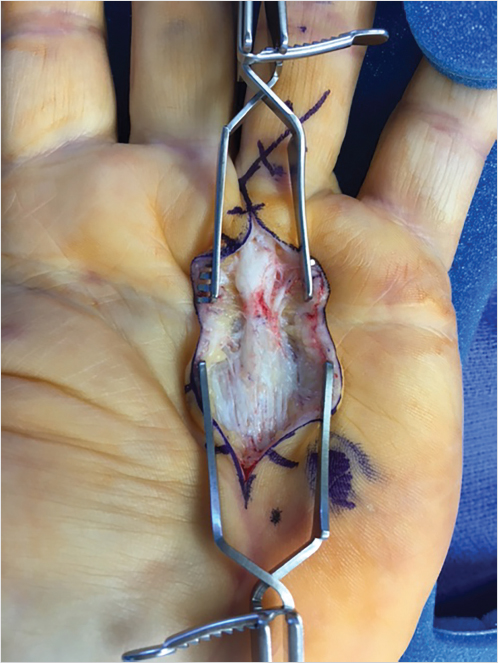
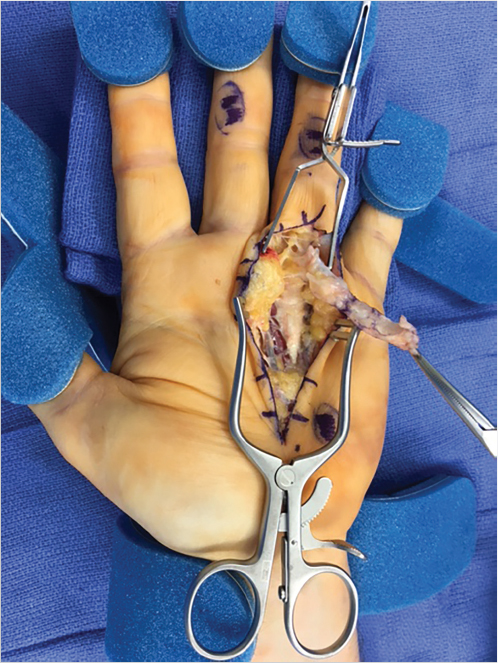
Fasciectomy is the most common surgical intervention in which all the macroscopically diseased tissues are excised (Fig. 29‑4). 5 , 6 , 7 Recurrence rates range in the literature from approximately 12 to 73% likely due to remaining microscopic diseased tissue. 2 , 3 It is difficult to interpret recurrence rates in the literature due to lack of standard definitions for recurrence. 2 , 3 , 8 Limited open or percutaneous fasciotomy was originally recommended for elderly or debilitated patients or patients who cannot participate in appropriate postprocedure rehabilitation, as they were thought to provide smaller power of correction. However, studies show percutaneous fasciotomy to provide excellent improvement with upward of 72% of MCP joint correction maintained over a 3- to 6-year follow-up period in a series reviewed by Pess et al. 8 PIP joint correction was less well maintained in the long term in their series of more than 1,000 digits. They concluded that percutaneous needle fasciotomy was a safe intervention method but resulted in a larger recurrence rate than open fasciectomy. 9
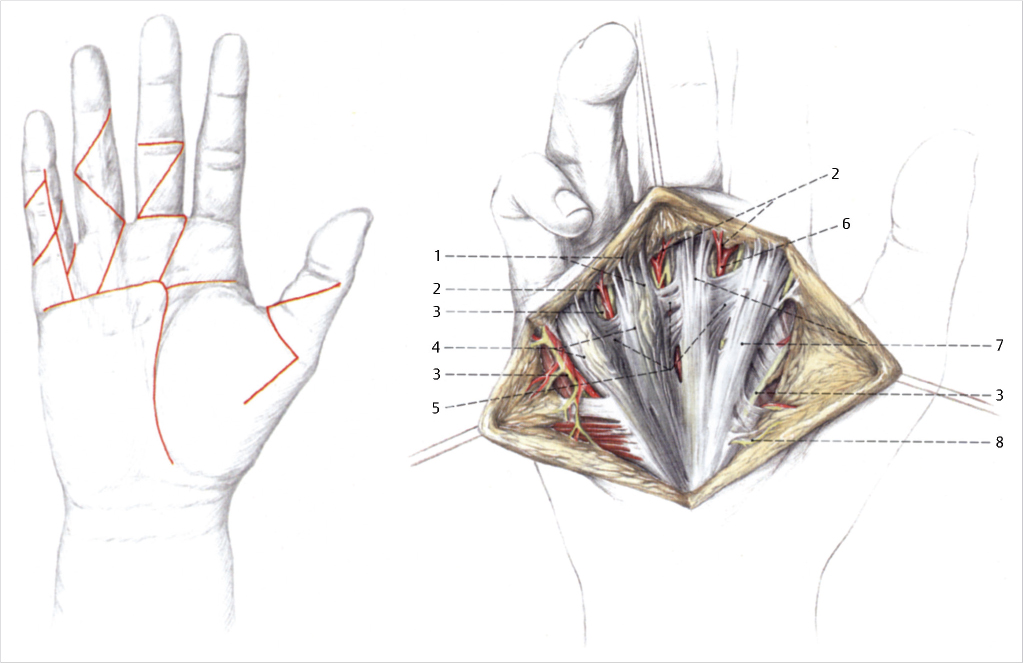
Palmar skin management after surgery is treated in three ways: direct closure, full thickness skin grafting, and open technique described by McCash allowing for skin closure by secondary intention through a transverse incision at the mid-palmar crease and then counter incision(s) in the digit(s) being addressed. The biggest complication of primary closure is the risk of postoperative hematoma and subsequent skin edge necrosis. Various incision types can be used including the aforementioned transverse incision as well as a midaxial longitudinal incision which is closed by forming multiple Z-plasties at the flexor creases or Bruner’s incisions with excellent exposure (Fig. 29‑5). Recurrence necessitating revision surgery is challenging and fasciectomy is recommended. However, the risk of neurovascular injury with devascularization of the digit must be considered. This is at higher risk for recurrent surgery due to the possibility of occult digital artery injury at the primary operation which could have been compensated for by the contralateral vessel. As such a new neurovascular injury could lead to a devascularized digit. Some authors have advocated that percutaneous fasciotomy technique can be utilized in the recurrent patient setting as well. Joint fusion may also be considered in selective cases of the MCP and/or the PIP in settings of painful arthritis, deformity over 90 degrees, dysvascular digit, and patient’s preference. 10
In recent history, the newest and increasingly more popular treatment for Dupuytren’s cases is the collagenase injection, Clostridium histolyticum (Xiaflex, Auxilium Pharmaceuticals). The collagenase is injected directly into the palpable cord in an office-based procedure and then typically between 24 and 48 hours after the injection, a finger extension manipulation is performed in the office to correct the contracture. The patient is fitted with an extension night time splint to wear for 2-4 months and with daily flexion exercises. The collagenase is approved for both MCP and PIP contractures with an overall recurrence rate (greater than 30 degrees worsening) at 5 year follow up of 26% for MCP joints treated, and 46% of PIP joints treated with an overall recurrence percentage of 47%. Also at 5 years, 16% of treated joints underwent secondary procedures for re-correction of contracture and the most common of which was surgical fasciectomy. 11 Collagenase is a favorable option for many Dupuytren’s patients with the proper counseling of recurrence rates and possible complications, the most common of which are swelling and ecchymosis to the hand from the injection followed by skin tearing after the manipulation which is treated with simple dressing changes alone. 12
29.3 Postoperative Care
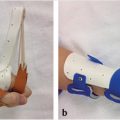
After surgical excision of the fascial bands, patients are splinted in extension with forearm-based splints, which can be transitioned to removable splints during the first postoperative week. All fingers are splinted in extension to minimize web-space contracture. Occupational therapy is initiated with passive and active range-of-motion exercises for both flexion and extension with passive extension stretching as well. By the second postoperative week, the patients can be weaned to night splinting while encouraging daily home exercises, but splinting usually will last 3 to 6 months. In the case of the McCash technique, patients are covered with a nonadherent dressing in the immediate postoperative period followed by daily dry dressing changes once motion is initiated at 1 week. Strengthening is delayed to approximately 6 weeks in these patients, while it can be initiated by 3 to 4 weeks postoperatively in other techniques.
29.4 Outcomes
Studies show that greater initial correction and PIP joint correction (if applicable) correlate with improved results and hand function at 6 and 12 months of follow-up. 6 , 13 In a natural history study of patients presenting with nodular disease, Reilly et al followed up 59 patients for 8 years with 30 of 59 patients developing cords; however, only 5 patients meet the criteria for surgical correction and only 3 of those 5 went on to surgery. 10 The primary risk of open fasciectomy is digital artery and/or nerve injury along with hematoma. Risks of percutaneous fasciotomy include skin tears (approximately 3%) and higher recurrence. 7 Collagenase injections have risk of local skin injury such as skin tears and blood blistering which has been reported in up to 46% of patients. Patient education should be held by the surgeon regarding various treatment options related to recurrence rates and risks of intervention to make the surgical decision a very personalized one for patients suffering from Dupuytren’s disease.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


