Abstract
This chapter addresses the diagnosis and anatomy of the different kinds of nerve compression that cause numbness, tingling, pain, or weakness primarily in the hand. Presurgical considerations are detailed, and surgical options, including open and endoscopic approaches, are discussed for each type of compression (e.g., carpal tunnel, median nerve, cubital tunnel, ulnar tunnel). Postoperative guidelines are provided, and there is an extended discussion of possible outcomes.
27 Nerve Compression Syndromes of the Upper Extremity
27.1 Goals and Objectives
Recognize the presentation of patients with upper extremity nerve compression syndromes.
Understand the anatomy of the different kinds of nerve compression.
Verify the location of the compression through physical exam and diagnostic tests.
Know when to offer treatment for a diagnosis of nerve compression.
Recognize postoperative complications and recurrence of nerve compression.
27.2 Patient Presentation
Patients with nerve compression will usually present to their primary care provider with weeks to months of hand “numbness,” “tingling,” “pain,” or “weakness.” Upon further questioning, the symptoms may wake them up at night or be present in the early morning hours upon awakening. The patients may relate the symptoms to certain activities that place tension or compression on the peripheral nerves such as driving, writing, keyboarding, shaving, hairstyling, or holding the phone to his ear. The symptoms may have developed with a change in medical condition such as pregnancy, hypothyroidism, or synovial proliferation, or with an increase or change in work or hobbies. More often than not, however, the condition is idiopathic; there is no clear etiology for the symptoms. The two most common forms of nerve compression are compression of the median nerve at the wrist (carpal tunnel syndrome) and compression of the ulnar nerve at the elbow (cubital tunnel syndrome). The examiner does need to be suspicious of the less common nerve compression syndromes involving the median nerve in the forearm (anterior interosseous and pronator syndrome), ulnar nerve in the wrist (ulnar tunnel), and radial nerve in the forearm (posterior interosseous syndrome, radial tunnel syndrome, and Wartenberg’s syndrome).
Physical exam consists of a visual inspection of the hand. Muscle wasting of the interosseous muscles indicates long-standing compression of the ulnar nerve. Wasting of the thenar muscles indicates severe medial nerve compression. Observe how the patient holds his digits; a claw-like (Duchenne’s sign) or flattened (“ape hand”) appearance indicates severe or prolonged nerve injury. It is more common for patients to present at earlier stages of compression. The examiner will look for signs of nerve “irritability” by tapping on the point of compression and eliciting the “Tinel’s” sign. This is found by tapping at the suspected point of compression, which is the distal wrist crease for carpal tunnel or the inside of the elbow for the ulnar nerve. Be aware that there is no standardization and considerable inter-examiner variability exists with this test. 1 The examiner may be able to elicit a positive “Phalen’s” test to the carpal tunnel by having the patient flex the wrists and increasing the pressure in the carpal tunnel. Digital pressure over the median nerve at the wrist is known as “Durkan’s” test and will reproduce the symptoms of carpal tunnel. The symptoms of cubital tunnel can be reproduced by having the patient fully flex the elbows while the examiner places digital pressure on the nerve.
The patient is asked to abduct and adduct his or her fingers to the examiner’s resistance and to cross and uncross fingers. Patients with significant ulnar nerve compression may have difficulty with this exercise. The patient is asked to abduct his or her thumb over and across the palm against resistance. Patients with median nerve compression and thenar muscle involvement may have difficulty with this maneuver.
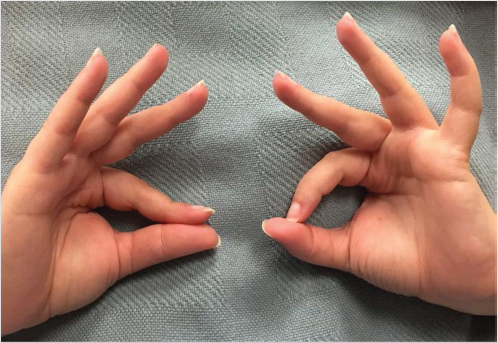
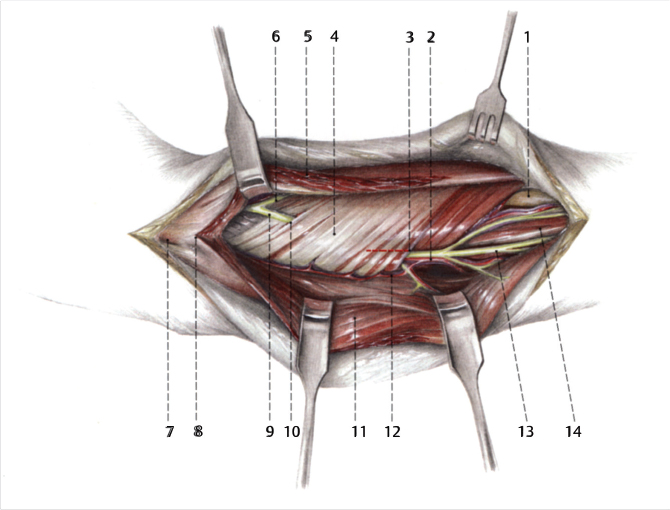
Anterior interosseous syndrome is a less common but well-described median nerve compression in the forearm. It presents as pain in the forearm and weakness of the innervated muscles (flexor digitorum profundus to the index and middle fingers, pronator quadratus, and flexor pollicis longus) without a sensory deficit. It can be identified on physical exam with a positive Tine’s sign over the fibrous bands in the volar forearm. The patient may fail the “pinch test” and not be able to make an “OK” sign with his thumb and index finger due to weakness in the proximally innervated muscles: flexor pollicis longus (index) and flexor digitorum profundus (Fig. 27‑1). Anterior interosseous nerve (AIN) syndrome can be confused with pronator syndrome, which presents as forearm pain and sensory disturbance in the median nerve distribution. Provocative tests for pronator syndrome include resisted elbow flexion, resisted middle finger flexion, and resisted forearm pronation.
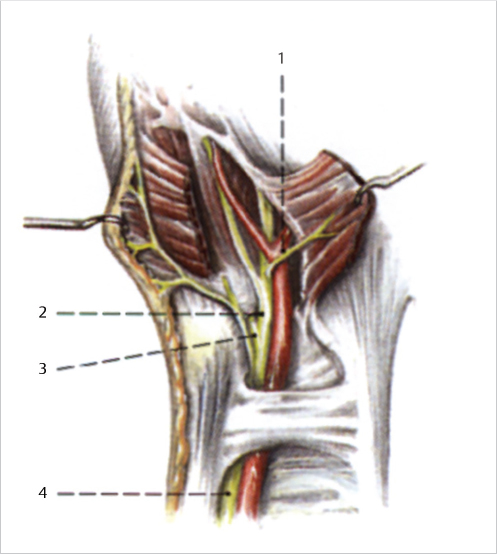
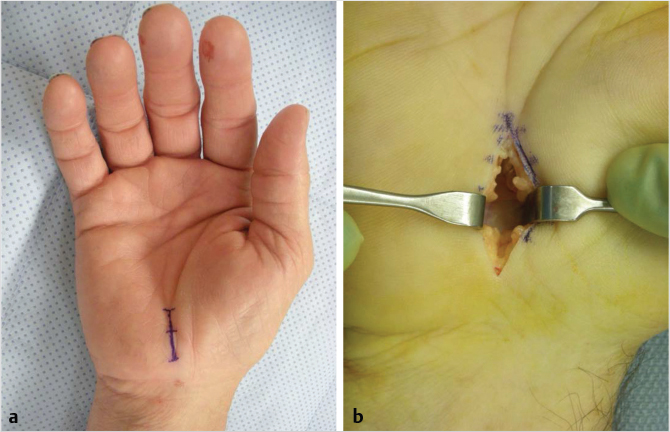
Ulnar tunnel syndrome is a compression of the ulnar nerve at the wrist. The ulnar tunnel, also known as Guyon’s canal, is divided into three zones and contains both the ulnar nerve and the radially located ulnar artery (Fig. 27‑2). Zone 1 is the most proximal and the patients will have sensory and motor symptoms. Zone 2 is radial and involves the motor branch of the ulnar nerve. Zone 3 is ulnar and the symptoms will be sensory. Guyon’s canal is bordered by the transverse carpal ligament (TCL) below and the volar carpal ligament and pisohamate ligament above. The most common reason for ulnar tunnel syndrome is a ganglion cyst (Fig. 27‑3). 2 An ulnar artery aneurysm or hook of the hamate fracture can also cause compression in this tight space. Ulnar tunnel syndrome can be distinguished from cubital tunnel syndrome by retained sensation over the dorsal/ulnar hand due to the takeoff of the sensory branch of the ulnar nerve proximal to the ulnar tunnel.

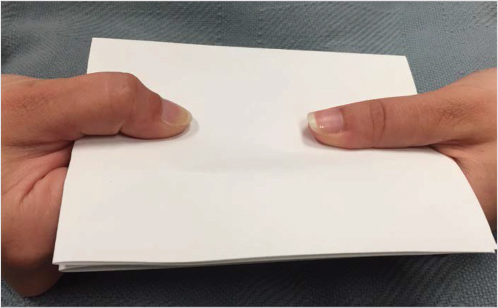
Additional physical exam findings can be noted with ulnar nerve compression. Patients will hold an object, such as a piece of paper, in the first web space by flexing the IP joint using the unaffected flexor pollicis longus instead of using the weakened adductor pollicis. This is known as “Froment’s sign” (Fig. 27‑4). The patients may not be able to adduct the small finger with the weakened palmar interosseous muscle due to the unopposed extensor digit quinti, innervated by the radial nerve. This is known as the “Wartenberg’s sign” (Fig. 27‑5).

Radial nerve compression can be found in the distal and proximal forearm. Distally, it is known as “Wartenberg’s syndrome.” Wartenberg’s syndrome is a compression of the superficial sensory radial nerve between the extensor carpi radialis and the brachioradialis. Patients will complain of pain, numbness, and paresthesias over the distribution of the radial sensory nerve. Blunt trauma over the radial/dorsal forearm or tight compression, such as a watch or handcuffs, can provoke this syndrome due to the superficial location of the nerve. Patients will avoid direct contact with clothing sleeves, gloves, or jewelry at the wrist. Symptoms can be provoked with flexion, pronation, and ulnar deviation of the wrist. This can be confused with de Quervain’s stenosing tenosynovitis, which can be present simultaneously; however, a distinguishing feature is that Wartenberg’s syndrome is present at rest. 3
Proximal radial nerve compression is known as “posterior interosseous syndrome” or posterior interosseous nerve (PIN). The patients present with complaints of pain in the forearm and weakness of the radial nerve innervated muscles. The patient will have wrist and metacarpophalangeal joint extension weakness. PIN palsy will need to be distinguished from extensor tendon rupture or tendon subluxation by examining for extensor tenodesis and the ability to hold digits already placed in extension. Radial tunnel syndrome is distinguished from PIN with a presentation of pain without motor or sensory disturbances. Symptoms can be provoked with resisted wrist supination or when traction is placed on the nerve by extending the elbow, pronating the arm, and flexing the wrist. Tenderness is found along the mobile wad.
Office-based equipment can help establish a baseline of the patient’s weakness and function. The two-point discriminator is a small pocket device used to examine the patient’s sensory loss. Normal two-point is 5 to 6 mm. 4 The patient’s grip and pinch are measured and compared with the other side using dynamometers. Traditionally, the dominant hand was believed to have a 10% greater grip; however, the difference may be minimal if the patient is left-handed. 5
Once the history and physical exam is completed, the patient will be asked to continue with diagnostic studies to verify the location of the suspected nerve compression. Nerve conduction studies (NCSs) and electromyography (EMG) are performed by a neurologist or physiatrist. NCS allows the examiner to accurately localize a lesion or identify a generalized disease process.
The EMG uses a needle to determine the health and function of the muscles innervated by the nerve in question. Generally, “mild” findings indicate prolonged sensory latencies with normal motor studies; “moderate” findings indicate abnormal sensory latencies and prolongation of median motor distal latencies; and “severe” findings indicate evidence of axonal loss. 6 These studies are helpful by not only verifying the location of the compression but ruling out other more serious, central problems that a plastic surgeon may not recognize such as amyotrophic lateral sclerosis, radiculopathy, or myasthenia gravis. 7 These studies can determine the severity of compression such as progression to muscle involvement. The EMG also serves as a baseline in the event of a patient deciding to pursue nonoperative treatment or presents postoperatively with complaints of worsening or ongoing symptoms. Due to variability in diagnostic equipment and examiners, we recommend having a relationship with a particular physiatrist or group who consistently performs your patients’ studies. Postoperative studies are expected to show electrophysiological improvement. 8 , 9
X-rays are easy to obtain and are not mandatory; however, the authors prefer to use them to identify or rule out coexisting pathology such as an occult fracture or osteoarthritis that may be contributory to the compression or become symptomatic during the postoperative period. A computed tomography or magnetic resonance imaging (MRI) may be indicated if a mass-occupying lesion is suspected as the etiology for PIN or AIN syndrome. An MRI is useful to differentiate a ganglion cyst from an aneurysm at the wrist.
27.3 Preparation for Surgery
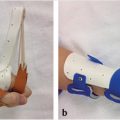
Patients are offered surgical decompression if they are healthy enough to tolerate surgery, are symptomatic, and have evidence of compression on the diagnostic studies. Surgery is most often performed using local plus intravenous sedation for the distal nerve compressions (carpal tunnel and radial sensory) or a regional block for compressions at the elbow or forearm. If the NCS or EMGs are read as “borderline,” “mild,” or do not indicate compression, conservative treatment is recommended. Conservative treatment for carpal tunnel involves nighttime splinting to prevent prolonged compression on the nerve from wrist flexion while sleeping. A steroid injection at the distal wrist crease adjacent to the median nerve can control or reduce symptoms. Studies have found that patients who respond well to steroid injections also tend to respond well to surgery. 10 We discuss risks such as skin depigmentation in darkly pigmented patients and elevated blood glucose levels in diabetics up to 5 days postinjection (Fig. 27‑6). 11 , 12 Conservative treatment for cubital tunnel syndrome involves elbow padding during the daytime to prevent inadvertent leaning on the nerve and antecubital padding at nighttime to prevent full elbow flexion that creates prolonged ulnar nerve tension during sleep.

Basic preoperative laboratory tests include a complete blood cell count, coagulations, and a basic metabolic panel. In the event that a patient is on Plavix, Coumadin, or ASA for a cardiac or neurologic reason, the authors will perform indicated hand surgery without stopping anticoagulation. Recent hand literature supports maintaining a patient’s anticoagulation regime, if that is in the patient’s best interest, with a low risk of complications. 13 , 14 , 15 The anesthesiologists often do regional blocks for patients on anticoagulants due to their skill in locating the brachial plexus with ultrasound. We offer in situ release of the cubital tunnel on anticoagulated patients to minimize dissection and bleeding risk. Nerve compression tends to be a chronic, not an acute, problem, and the authors recommend allowing any unresolved medical problems to be addressed first in the best interest of the patient.
Elective hand patients need to have their diabetes and hypertension under control before committing to surgery to avoid postoperative systemic and local complications. 16 , 17 HbA1c levels can be used to identify patients with poor glycemic control. Values between 6.5 and 8% have been recommended. 18 Antihypertensives are usually continued until the day of surgery. Patients with systolic blood pressure ≥ 180 mm Hg or diastolic blood pressure ≥ 110 should have their pressures lowered gradually over days to weeks as outpatients. 16
In the event of bilateral compression, one side will be offered, followed by the other side 4 to 6 weeks later. Patients often request bilateral surgery for the sake of time and convenience, but we remind patients that one side has to be free to perform activities of daily living, while the other side can be allowed time to heal while staying clean and dry.
Wartenberg’s syndrome, radial tunnel syndrome, and pronator syndrome do not tend to have objective findings on nerve studies. These cases would be best served with conservative treatments of nonsteroidal anti-inflammatory drugs (NSAIDs), activity modification, and splinting for 3 to 6 months. A diagnostic lidocaine injection at the point of compression can help with future surgical planning and expectations.
27.4 Treatment
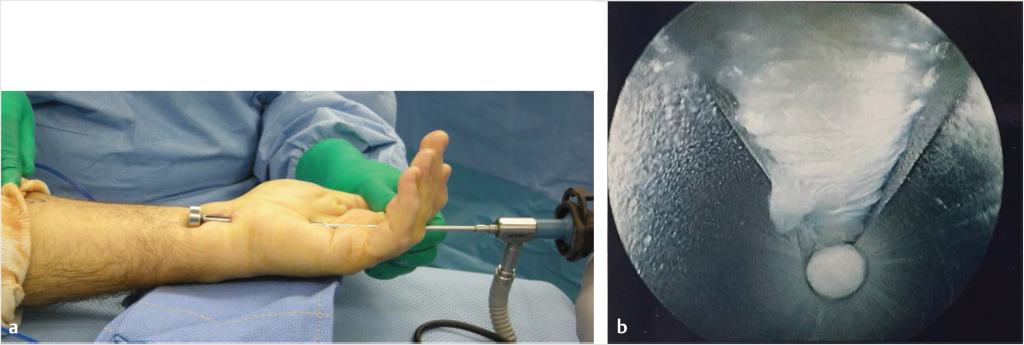
The surgical treatment of carpal tunnel syndrome is simple decompression of the TCL. This can be done through an open approach (Fig. 27‑7) or endoscopic approach (Fig. 27‑8). The most popular option is the open release, which requires less specialty training and has a shorter learning curve. 19 The advantage of the endoscopic release is an earlier recovery and return to work. The skin incisions are shallower, allowing for a faster recovery time. Results have been similar over the long term, ranging from 3 months to 1 year. 20 , 21 , 22 , 23
During open release, synovectomy and manipulation of the nerve are not indicated except for specific cases of synovial hypertrophy that need debulking. A forearm-based tourniquet is well tolerated and is set to 225 mm Hg after manual exsanguination. We recommend a median nerve block using 1% lidocaine and 0.25% Marcaine placed at the distal wrist crease in preoperative holding to allow time for the medication to work and dissipate from the surgical site. The carpal tunnel can be released under direct vision by making a longitudinal incision over and through the TCL from the volar wrist flexion crease, staying in line with the radial border of the fourth ray. Visualization of the palmar fat is the distal end point. A tenotomy scissors can be used to release the distal end of the antebrachial fascia in the forearm, staying ulnar to the palmaris longus tendon. The TCL is about 2 cm in length. The days of large palmar and forearm dissections are long gone and unnecessary, and only contribute to prolonged recovery and scar adhesions.
The endoscopic carpal tunnel release is a minimally invasive alternative to the open release. This is most often performed proximally based, using either a single or double port. An upper arm tourniquet set at 250 mm Hg after manual exsanguination is necessary. A distally based flap of antebrachial fascia is elevated at the distal wrist crease through a transverse incision just above and ulnar to the palmaris longus tendon. A spatula is used to bluntly remove the synovial tissue from the undersurface of the TCL. An endoscopic 4-mm 30-degree camera is placed distally to visualize the TCL. The edge of the ligament is verified with a blunt hook. A sharp hook is used to transect the ligament under endoscopic vision in a distal to proximal direction.
Postoperatively, the patients are placed in a bulky dressing and encouraged to use their fingers while avoiding lifting or gripping more than 5 lb for 4 to 6 weeks. Open carpal tunnel releases are splinted for a week if they give indication that they are at a higher risk of wound breakdown. Patients are brought back within 10 days for suture removal and one hand therapy visit to assist with mobility and scar management.
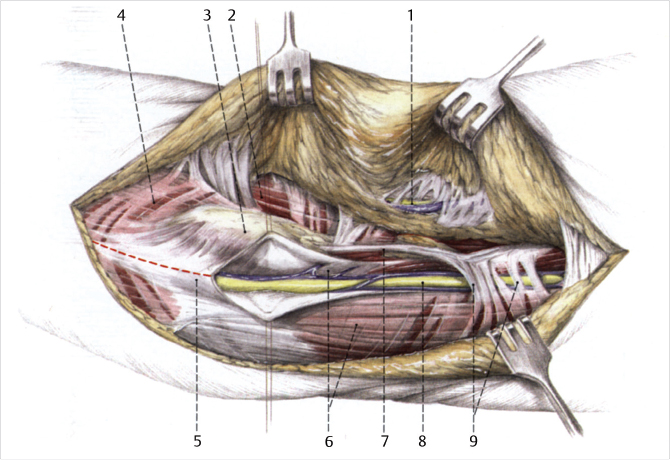
Median nerve decompression at the forearm requires an upper extremity tourniquet and regional block. A lazy S incision is made from just proximal to the antebrachial fossa to the mid-volar forearm. Points of compression needing to be identified and released or lengthened, from proximal to distal, are ligament of Struthers, bicipital aponeurosis, tendon of the superficial head of the pronator teres, deep head of the pronator teres, and arch from the leading edge of the flexor superficialis (Fig. 27‑9). The patient is placed in a bulky dressing restricting full elbow mobility until sutures are removed. Controversy exists over when surgical intervention is appropriate. Most authors recommend surgical decompression after 3 months of conservative treatment or persistent findings on electrodiagnostic studies. There have been reports of spontaneous recovery, but an inflammatory etiology may have been responsible for the AIN palsy. 24
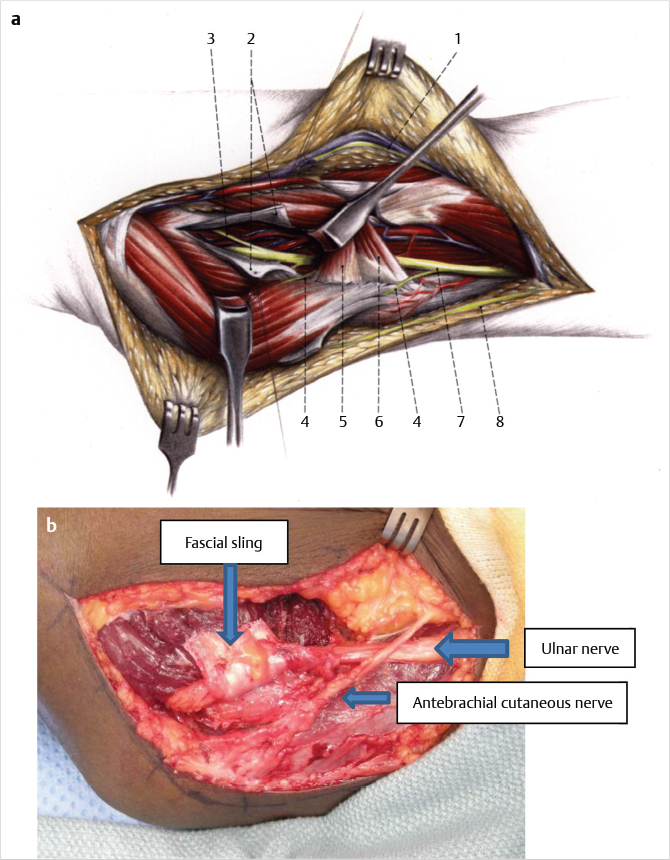
There are many accepted alternatives for cubital tunnel release. They include open in situ; subcutaneous, intramuscular, transmuscular, and submuscular transposition; medial epicondylectomy; and endoscopic in situ. The points of compression have to be identified and addressed. These include (proximal to distal) arcade of Struthers, intermuscular septum, Osborne’s ligament, anconeus muscle (if present), and the flexor pronator fascia (Fig. 27‑10). Care needs to be taken to identify and protect large crossing branches of the antebrachial cutaneous nerve, found on average 1.8 cm proximal and 3.1 cm distal to the medial epicondyle as well as the motor branch to the flexor carpi ulnaris (FCU) muscle, located distal to the medial epicondyle. 25 The authors prefer to anteriorly transpose the nerve over the medial epicondyle using the subcutaneous or transmuscular techniques to avoid tension on the nerve during elbow flexion. Dissection of the nerve can temporarily devascularize it, but no correlation has been found between devascularizing the nerve during transposition and postoperative nerve recovery. 26 We offer open in situ release to patients who are less than optimal surgical candidates for the sake of speed and simplicity. Median epicondylectomy is another option that has been found to be successful; however, the authors prefer to avoid the risks of bone tenderness, elbow instability, and heterotopic bone formation.
Postoperatively, we splint patients for 1 week in a padded elbow splint. One to two visits with hand therapy is usually sufficient to recover elbow mobility. Submuscular transposition requires a longer splinting protocol, risking elbow stiffness, which is why it is not our first-line treatment.
Patients with ulnar tunnel syndrome are given a regional block and a forearm tourniquet. The incision is made in a zigzag fashion using the FCU, pisiform, and hook of the hamate as landmarks. The ulnar nerve runs radial to the FCU and between the pisiform and hook of the hamate. The nerve is identified, taking care to identify and protect the ulnar artery. Dissection of the nerve continues until the aponeurotic arch of the hypothenar muscles is released. An anomalous structure, such as a ganglion, fracture fragment, or aneurysm, needs to be identified and removed. The patient is placed in a bulky dressing until return to clinic for suture removal within 10 days.
Spontaneous resolution is typically expected with Wartenberg’s syndrome that includes removal of the inciting etiology (compressive force), rest, splinting, and NSAIDs. 3 Surgery is offered after failure of conservative treatment. Decompression of the radial sensory nerve is performed under a proximal forearm tourniquet and can be done under local or regional block with sedation (Fig. 27‑11). A longitudinal incision is made over where the radial sensory nerve (RSN) presents between the brachioradialis (BR) and extensor carpi radialis longus tendons, located approximately 9 cm proximal to the radial styloid, staying slightly volar to avoid direct nerve contact. When operating near the RSN, we recommend breaking dermis only with the knife and doing longitudinal blunt dissection. Decompress the fascia between the tendons. Cover with a bulky dressing.
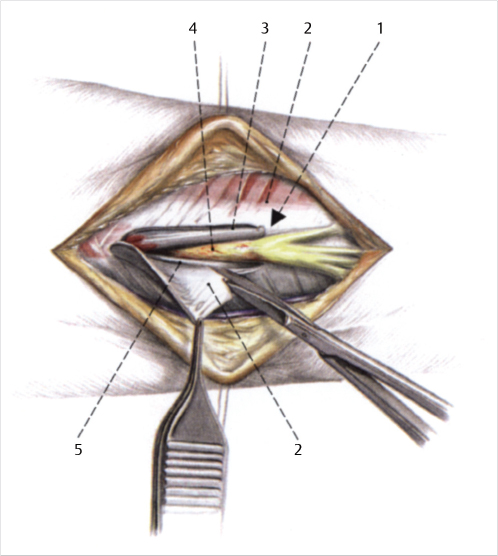
An initial trial of nonsurgical management of PIN and radial tunnel syndrome is recommended. This includes rest, splinting, and anti-inflammatories. An injection of lidocaine and a steroid may be diagnostic and therapeutic for radial tunnel syndrome. 3 If symptoms persist after 3 months, decompression of the PIN is considered. This is performed with an upper extremity tourniquet and under regional block. A longitudinal incision is made over the mobile wad, most easily found when the forearm is pronated on the operating table with the elbow gently flexed. Points of identification and decompression are fibrous tissue anterior to the radiocapitellar joint, “leash of Henry” (recurrent radial vessels), edge of the extensor carpi radialis brevis, arcade of Frohse (proximal edge of the supinator), and distal edge of the supinator (Fig. 27‑12). The arm is placed in a bulky dressing. We recommend surgical taping of the dorsal forearm scar for several months in the postoperative period to minimize scar hypertrophy.
All patients with regional blocks are sent home in slings with instructions to remove the sling once sensation and motor function returns. This is to avoid a stiff shoulder.
The use of perioperative antibiotics has not been found to be indicated in elective, clean hand cases. 27 We do give immunocompromised patients, such as diabetics or those on steroids, one perioperative dose of antibiotics before tourniquet inflation. These are clean cases and the antibiotics are not continued in the postoperative period.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


