Abstract
This chapter deals with a significant trauma that remedially requires the rapid processing of many issues. Surgery is based on the findings of medical, laboratory, and radiologic evaluations; factors that enhance the possibility of success (e.g., wrapping the amputated digit in moist gauze, sealing it in a plastic bag that is placed on ice) are covered, and surgical contraindications are enumerated. The examination of affected bones, tendons, nerves, arteries, and veins is described, and if surgery is deemed possible, the recommended techniques and procedures (including the use of leeches) are sequentially listed. Because postoperative care for both replantation and amputation is critical, the authors conclude their study by going into some detail about practices that increase the odds for a satisfactory outcome.
28 Replantation and Amputation of Fingers
28.1 Goals and Objectives
Review the indications for replantation and amputation of fingers.
Outline technical aspects of finger replantation and amputation.
Summarize reported outcomes and evidence-based recommendations for management of fingers evaluated for replantation or amputation.
28.2 Patient Presentation
In the setting of traumatic amputations involving one or more fingers, decisions regarding replantation and amputation have complex implications for patients. It is necessary for patients and surgeons to work through many issues in a relatively short period of time to determine an optimal treatment plan.
Initial evaluation must include an examination of the injured parts (including physical examination and X-ray), review of the mechanism of injury, and thorough assessment of any associated injuries and coexistent medical problems. 1 , 2 , 3
If a patient is first seen in a facility which will transfer the patient elsewhere for definitive management, primary emergency care should include dressing and elevation of the injured hand; wrapping of the amputated parts in moist gauze and subsequent placement into a specimen cup or plastic bag which is then placed on ice; establishment of intravenous access in an uninjured extremity; evaluation of medical problems and associated injuries; performance of indicated laboratory and X-ray studies; and administration of indicated antibiotics, analgesics, and tetanus prophylaxis. If the patient presents to the same hospital where definitive care will be offered, the responsible hand surgeon can directly oversee this primary management.
With accomplishment of initial evaluation, the surgeon can examine the amputated parts. The patient and surgeon then must arrive at a treatment plan.
Replantation can offer possibilities of maximum salvage of function with the drawbacks of prolonged surgery and hospitalization as well as prospects of lengthy postoperative therapy and secondary procedures. Each patient will have individual priorities to bring to the formulation of a surgical plan; each injury will offer the surgeon a range of possibilities and limitations. These elements must be assembled into the best available composite of patient expectation and surgeon performance.
The indications for replantation have been established over decades. Prime opportunities for replantation based on prospects for useful salvage of function include amputation of thumbs, multiple fingers, amputations in children, and finger amputations distal to superficialis tendon insertion. Contraindications can include crushing and multilevel amputations and single-finger injuries proximal to the superficialis insertion. Specific patient issues, including commitments to recovery time, can ultimately determine the surgical plan. 4
If replantation is not a consideration, or if intraoperative findings or postoperative failure aborts a replantation effort, the surgeon must apply effective amputation strategies.
28.3 Treatment
28.3.1 Preparation for Surgery
Review of the preparations described earlier, including medical, laboratory, and radiologic evaluations, forms the basis for proceeding to surgery. Radiographs of the hand will provide information regarding the level and extent of bone and/or joint trauma. Similarly, radiographs of the amputated part may be desired.
Informed consent should include options for amputation as well as replantation procedures that could include vein, nerve, and skin grafts, as well as anticoagulant use and blood transfusion.
The patient should be further informed of the duration of surgery and hospitalization, risks of replant failure, length of recovery, and possible need for secondary operations.
28.4 Replantation
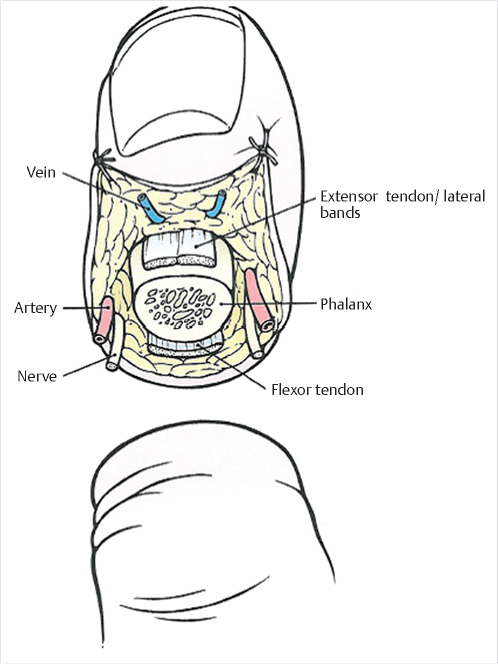
Initial exploration of the amputated digit includes examination of bone and tendons, as well as identification and tagging of digital nerves, digital arteries, and volar veins. These maneuvers are facilitated by making midlateral incisions in the digit, allowing reflection of dorsal and volar tissue to create a wide field (Fig. 28‑1).
The injured hand is explored under tourniquet control. Proximal incisions are made, usually in a Bruner pattern, to identify and tag critical structures to match the components prepared in the amputated part. 5
Generally, replantation of multiple digits is prioritized from thumb to ulnar digits with the index finger being the most functionally expendable. 6 A cleanly amputated part can be replanted at a more optimally functional site if that site’s amputated part is unreplantable. For example, a cleanly amputated index finger can be replanted onto a thumb site when the amputated thumb itself is not replantable. 7
Replantation follows an organized sequence of bone fixation, volar repairs (flexor tendons, digital arteries, digital nerves, and skin closure), and dorsal repairs (extensor tendon, veins, and skin closure). 4 , 6
A number of skeletal fixation techniques have been used in replantation, but crossed Kirschner wires (K-wires) offer speed of application and simplicity of technique with no documented outcome disadvantages relative to more complicated systems. K-wires can be placed through the amputated part at the initial dissection. Replantation can then commence with reduction of the amputated bone into the proximal skeletal stump, usually under direct visualization. The K-wires are then driven into the proximal bone. Wire position and reduction can be confirmed by fluoroscopy. 4 , 6 , 8
Flexor tendon repairs are performed next. At the initial exploration, sutures can be placed in the proximal and distal tendon stumps with each suture representing one half of the selected tendon repair technique. Completion of the repair is accomplished by tying the two segments of sutures together. 4 , 9
The tourniquet is released following skeletal and flexor tendon repairs. Under the microscope, the digital arteries and nerves are examined. The proximal and distal margins of these structures are trimmed to grossly uninjured levels. The proximal artery should be treated with mechanical dilation, heparin irrigation, and topical vasodilation (e.g., papaverine) until pulsatile flow is identified. The digital artery segments are then anastomosed, usually with 9–0 or 10–0 nylon sutures. Repairs of both arteries should be considered to guard against failure of a single repaired vessel. Both digital nerves are next repaired using 9–0 or 10–0 nylon sutures. The volar skin is closed as loosely as possible. 4 , 6 , 9
Significant gaps in specific tissues can be addressed with grafts. Vein grafts can be used to bridge arterial defects. These grafts can be harvested from a foot, with veins near a web space being a good match for digital arteries while veins on the distal dorsum of the foot are generally suitable for common digital arteries. 10 Digital nerve gaps rarely have sufficiently secured skin cover for the surgeon to consider autologous nerve grafts, but small vein conduits or cadaveric nerve allografts can be successfully applied. 11 , 12 Significant gaps in skin cover, including defects exposing underlying neurovascular repairs, can be covered with small split or thinned full-thickness skin grafts. 13
After completion of volar repairs, the hand is turned for access to the dorsal injury. The extensor tendon is repaired with absorbable sutures. One or more veins are then repaired, and vein grafts can be used here also. Veins can be identified during the initial dissection, but optimal distal vein selection is best accomplished after arterial repairs establish venous outflow from the amputated part. 4 Dorsal skin closure completes this procedure.
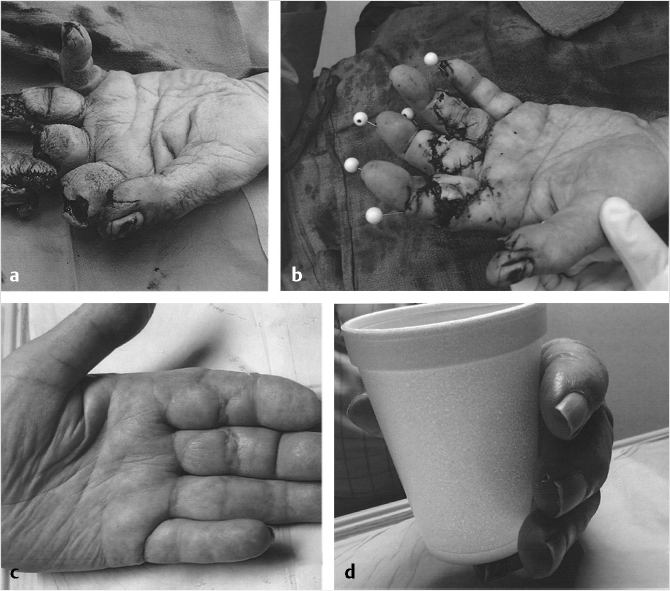
For multiple replantations, a functional operative sequence includes preliminary dissection and tagging of all proximal and distal structures; skeletal reduction; flexor tendon repairs; introduction of the microscope and tourniquet release; all arterial repairs; all nerve repairs; volar skin closure; and turning of the hand for all extensor repairs followed by vein repairs and dorsal skin closure (Fig. 28‑2). First priority for salvage should be given to the thumb, followed by little, ring, middle, and index fingers.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


