26 Periareolar Mastopexy Augmentation
Summary
This chapter summarizes an approach to periareolar mastopexy augmentation in the patient with mild-to-moderate ptosis questing augmentation mastopexy. It outlines a safe approach to the procedure with minimal risk to the overlying breast and optimizes outcomes in terms of shape retention and minimizing of areola stretching and scar hypertrophy. Technical pearls are included to help minimize risk. Clinical examples are provided to illustrate the technique and its outcomes.
Key Teaching Points
Periareolar mastopexy augmentation is reserved for minor degrees of ptosis remaining after breast augmentation has been performed.
Capsular contracture rates tend to be higher than those achieved with the inframammary approach.
Stretching of the areolar diameter and hypertrophic scarring are consistent problems with this technique.
Flattening of the front of the breast is a common problem.
26.1 Introduction
Periareolar mastopexy augmentation is designed for patients requiring minimal degrees of ptosis correction after breast augmentation. There are two approaches when performing this operation:
The entire augmentation is performed through the periareolar mastopexy incision.
The augmentation is performed through an intramammary approach while the mastopexy is performed through a separate periareolar incision.
Many patients seeking periareolar mastopexy augmentation desire the procedure so as to camouflage this scar within the areola margin. The addition of a separate inframammary incision may not be desirable in their eyes but does potentially reduce the risk of capsular contracture. The two approaches involve entirely different dissections for implant placement.
Pearl
One of the few major advantages in using the periareolar approach to mastopexy augmentation is that it is safer to perform a subfascial augmentation in combination with the periareolar mastopexy as the latter procedure does not involve wide undermining of the skin or the use of glandular flaps in order to achieve a breast lift. This ensures optimal retention of blood supply to both the gland and skin when the subfascial plane has been dissected.
26.2 Patient Selection
As has been mentioned above, the combination of periareolar mastopexy and augmentation is indicated primarily for patients with mild degrees of ptosis requiring augmentation. It should be remembered that any breast augmentation will achieve some degree of ptosis correction and this is particularly true when a subfascial approach is performed. This is due to the fact that subfascial implant placement allows for maximum impact of the implant’s projection upon the overlying breast’s shape. When the submuscular approach is used, the muscle tends to flatten the anterior projection of the implant to some extent, reducing its ability to lift the breast quite as effectively.
Periareolar mastopexy alone will only achieve an areolar lift of approximately 1 to 2 cm with any degree of reliability. It should be remembered that when combined with augmentation, the augmentation will achieve an element of mastopexy effect as well and the two procedures in combination can result in a breast lift of approximately 2 to 3 cm.
Pearl
Patients should be carefully selected as being only those who require minimal areolar elevation without any need for reduction in the transverse diameter of the breast. This may be achieved with either a vertical or Wise pattern mastopexy technique.
It should also be borne in mind, that if the patient requires reduction of a large areolar diameter in the first place, that the amount of skin removed to achieve a 1- to 2-cm areola lift must take the areola reduction excision into account. Failure to do so will result in excessive tension across the newly sutured leading to stretching of the areolar diameter once more, coupled with an increased tendency to hypertrophic scarring. Tension across the areolar diameter will also predispose the patient to flattening of the front of the breast resulting in a very unattractive long-term breast shape.
Pearl
As with all combined mastopexy augmentations, the augmentation must always be performed first. The skin excision should only be performed once the baseline tension of the breast has been set with implant placement. This will avoid excessive skin resection resulting in tension at closure.
Surgical Plan
Preoperative marking.
Periareolar incision.
Infra-areolar dissection.
Subpectoral dissection.
Parenchymal closure.
Periareolar mastopexy deepithelialization and closure.
26.3 Operative Technique
26.3.1 Incision
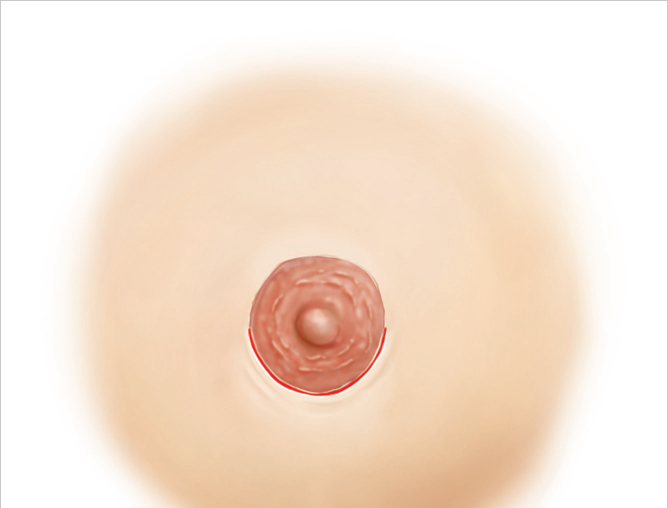
A periareolar incision should be placed directly at the junction between the outermost pigmented portion of the areola and the adjacent normal colored breast skin. Placing the incision within the areola may result in the pale scar within the pigmentation of the areola resulting in increased visibility. I usually use the inferior lower pole of the areola for such an incision from 9 to 3 o’clock position (▶Fig. 26.1).
26.3.2 Lower Pole Dissection
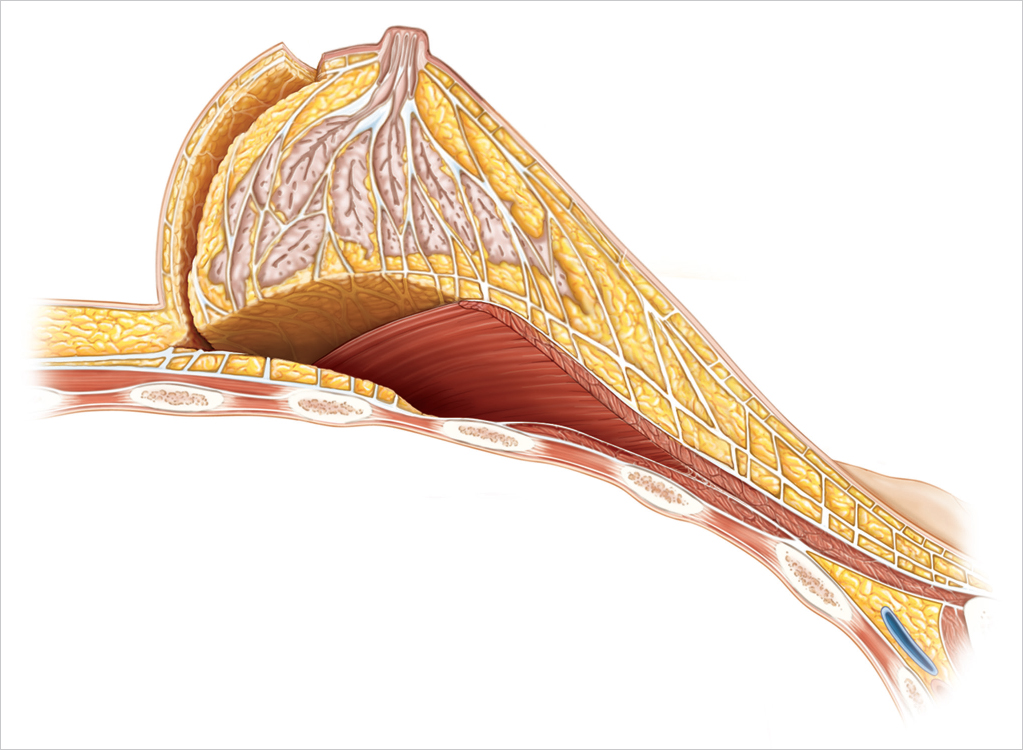
Dissection needs to be carried out to the lower pole of the breast gland at the inframammary crease. It can then proceed beneath the inferolateral border of the pectoral muscle to enter the subpectoral plane. In order to reach this plane, two approaches are feasible. I prefer to dissect subcutaneously to the 6 o’clock position, freeing up the breast between 5 and 7 o’clock position at the inframammary crease. This allows elevation of the lower pole of the breast in a cephalad direction, exposing the inferolateral border of the pectoralis major muscle for elevation (▶Fig. 26.2).
An alternative approach is to split the gland vertically along the 6 o’clock position meridian of the lower pole once the subcutaneous plane has been dissected. While this may allow for a wider exposure, it does create more bleeding and requires more suturing to repair the glandular defect in order to prevent the appearance of vertical grooving of the lower pole if the repair is inadequate.
26.3.3 Subpectoral Dissection
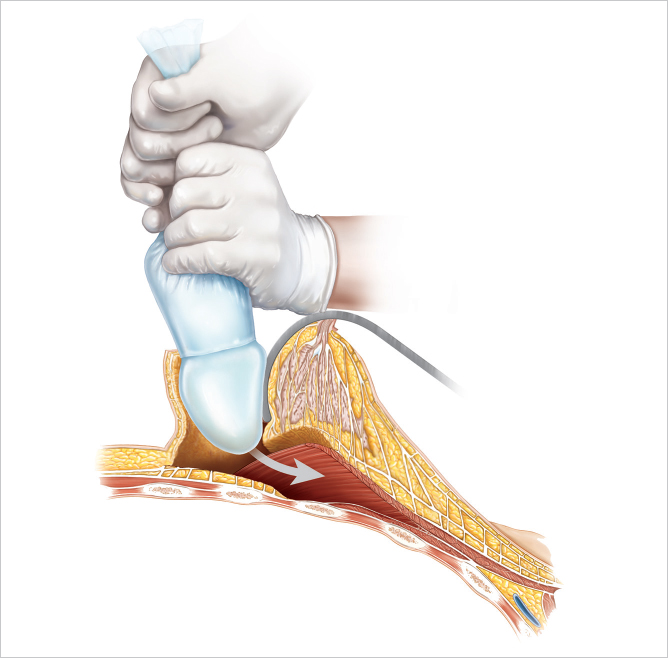
The subpectoral dissection is carried out in the usual manner described in the preceding chapters on subpectoral augmentation. It is somewhat more awkward to achieve given the retraction of the breast from the periareolar incision. The implants can then be placed in the usual manner, taking care to apply all of the 14-point principles described by Adams as a means of reducing biofilm contamination and subsequent capsular contracture (▶Fig. 26.3).
26.3.4 Parenchymal Closure
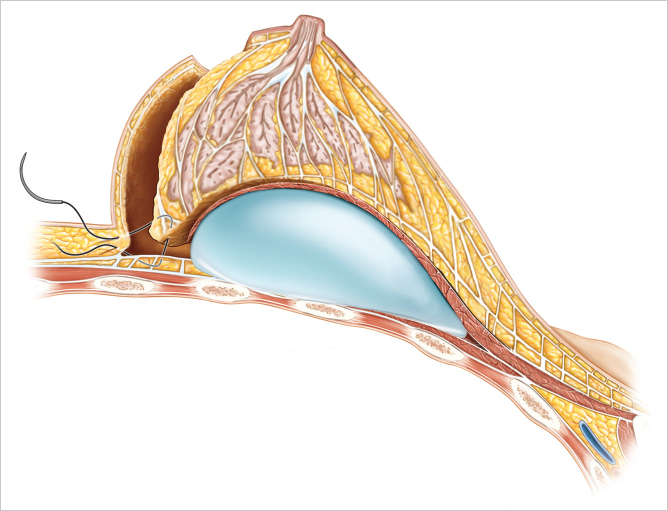
The breast gland should then be suited to the inframammary crease with interrupted or running vital sutures in order to close down the pocket and re-create the integrity of the inframammary crease (▶Fig. 26.4).
Related posts:
 25 Decision Making in Mastopexy Augmentation
25 Decision Making in Mastopexy Augmentation
 29 Prevention and Management of Complications in Mastopexy Augmentation
29 Prevention and Management of Complications in Mastopexy Augmentation
 28 The Wise Pattern Mastopexy Augmentation
28 The Wise Pattern Mastopexy Augmentation
 27 Vertical Mastopexy Augmentation
27 Vertical Mastopexy Augmentation
 16 Subfascial Inframammary Breast Augmentation
16 Subfascial Inframammary Breast Augmentation
 54 Prevention and Management of Complications in DIEP Flap Reconstruction
54 Prevention and Management of Complications in DIEP Flap Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


