29 Prevention and Management of Complications in Mastopexy Augmentation
Summary
Mastopexy augmentation is reviewed, highlighting its role as being one of the most complication-laden procedures in cosmetic breast surgery. The roles of tension, scarring, and vascular compromise are outlined in detail and methods to reduce complications are provided.
Key Teaching Points
Mastopexy augmentation is considered one of the riskiest procedures in aesthetic breast surgery.
Vascular complications are directly related to the degree of undermining and intraparenchymal dissection undertaken.
Tension is a major factor in causing skin necrosis.
Scarring and poor shape outcomes associated with this procedure are among the most common causes of litigation in breast surgery and, indeed, in plastic surgery as a specialty.
29.1 Introduction
Mastopexy augmentation is a powerful tool for reshaping and rejuvenating the female breast when correctly performed. It incorporates the risks of both mastopexy and augmentation which, when combined, can create the perfect milieu for surgical catastrophe. Much has been written about this complex procedure and many surgeons still advocate separating the two procedures to minimize risk, performing the mastopexy first followed later by an augmentation. While this approach may seem safe, it does require two anesthetics with their combined risk and creates a significant financial burden not seen in the single combined procedure. Combined single-stage mastopexy augmentation is my preference but requires careful planning and safe execution to achieve predictable results.
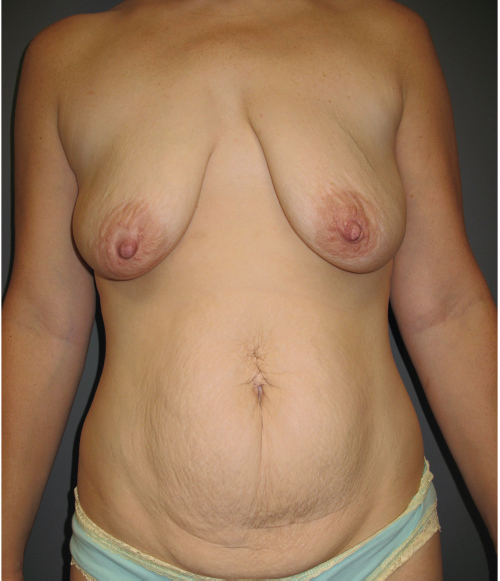
It requires good aesthetic sense and careful judgment to perform well. Failure to observe sound basic principles may result in potential disaster. It should be remembered that ptotic patients usually have skin and parenchyma that have inherently poor support; relying on this tissue alone for long-term support is likely to disappoint both patient and surgeon (▶Fig. 29.1).
29.2 Causes of Complications in Mastopexy Augmentation
Excessive undermining in the subglandular or subfascial plane with key medial perforator division.
Extensive intraparenchymal dissection to raise glandular flaps resulting in devascularization and fat and/or nipple and skin necrosis.
Closure of skin flaps under excess tension leading to necrosis or hypertrophic scarring. Failure to plan for the increased tension generated by the contained augmentation, having committed to skin excision before performing the augmentation.
Placing excessively large implants into a breast that has already demonstrated a propensity for stretching to take place.
Failing to place nonabsorbable periareolar sutures to limit areola stretch.
Failure to deal with vertical lower pole length resulting in abnormal breast proportions.
Relying on poor-quality local tissue support to correct problems with inframammary fold (IMF) asymmetries.
Asymmetry of implant placement and mastopexy.
29.2.1 Excessive Undermining in the Subglandular or Subfascial Plane with Key Medial Perforator Division
Breast blood flow remains the quintessential determinant of tissue viability following any breast procedure. Nowhere is this more imperative than in mastopexy augmentation. As was demonstrated in the Anatomy section of this text, the breast derives its vascularity from several major sources including the thoracoacromial, internal mammary, intercostal and lateral thoracic arteries, and their accompanying venous drainage. While the breast can survive on significant reductions in some of these vascular territories, it cannot withstand major vascular disruption without incurring tissue necrosis. Certain mastopexy techniques such as the Wise pattern approach generate relatively thin apical flaps at the inverted-T closure. The flap tips are less well perfused than their thicker proximal counterparts and any tension may tip the balance in favor of necrosis. In addition, some surgeons make use of extensively undermined parenchymal flaps, which may have a random pattern of perfusion rendering them more prone to necrosis.
Augmentation can also impair breast blood supply and this is particularly true of the subfascial approach as it results in elevation of the breast off the pectoralis major muscle, severing many of the smaller vascular contributions to breast blood supply from the underlying muscle. If medial perforators are then injured, major breast necrosis can occur (▶Fig. 29.2).
Technical Pearl
Every effort should be made to preserve breast blood supply. Care should be taken to preserve medial internal mammary perforators when dissecting toward the cleavage and these are particularly at risk during subfascial augmentation.
29.2.2 Extensive Intraparenchymal Dissection to Raise Glandular Flaps Resulting in Devascularization Causing Fat or Nipple Necrosis
Breast flaps should be kept short with minimal undermining to maintain blood supply, and if raised, shsould be done so on reliable pedicles. Length to breadth ratios should be kept to within a maximum of 3:1. Greater lengths may induce fat necrosis resulting in coarse calcifications visible on mammography. It should be remembered that these patients have already demonstrated a marked tendency for their parenchymal support to fail. The use of complex breast flaps to shape and hold the breast in position is likely to meet with little success in the long term. If extensive internal support is required, it is preferable to use some form of acellular dermal matrix (ADM) to act as an antigravitational sling. In this setting, I prefer porcine dermal matrices over human donors, as the porcine matrix has less potential for stretch.
While Vicryl absorbable mesh has been advocated, its use seems counterintuitive. Vicryl absorbs over 12 weeks and loses 50% of its tensile strength by 3 weeks, providing little in the way of support even in the short term.
29.2.3 Closure of Skin Flaps under Excess Tension Leading to Necrosis or Hypertrophic Scarring
Tension is the enemy of any plastic surgical procedure. It causes wound dehiscence, skin edge necrosis, and is an important trigger for both hypertrophic and keloid scar formation. Any mastopexy augmentation is at risk for tension-related issues but none more so than the Wise pattern with its right-angled flap tips. Mastopexy alone is a risk but combining the ptosis procedure with augmentation generates internal pressure that exacerbates the tension on the overlying skin envelope. This can lead to necrosis, wound dehiscence, implant exposure, and infection.
Technical Pearl
Skin flap tailoring should always be performed after augmentation. This sequence allows the surgeon to adjust the preoperative markings to accommodate the tension generated by the implant, leaving looser skin flaps for suturing without tension.
29.2.4 Placing Excessively Large Implants into a Breast that has Already Demonstrated a Propensity for Stretching to Take Place
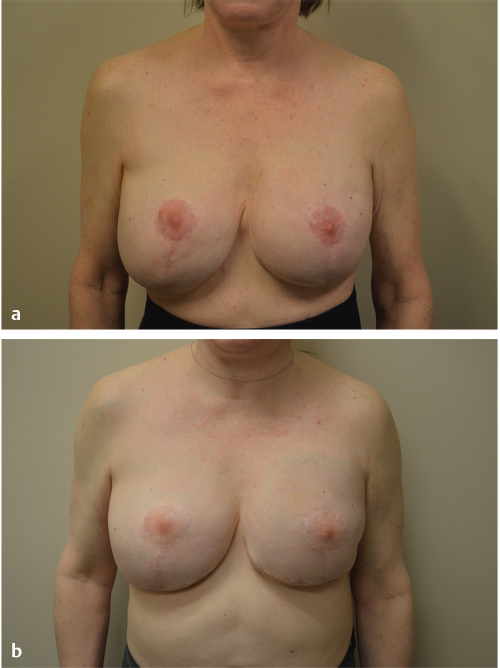
Breast augmentation increases the weight of the breast, which in turn causes gravitational pressure on the skin envelope. Excessive implant volumes result in heavy breasts that tend to sag over time, resulting in recurrence of the ptosis with which the patient initially presented. The larger the implant volumes, the greater this tendency to recurrent ptosis will be. In addition, large implants create significant disproportion in the final outcome despite a mastopexy, resulting in distortion of the normal 45:55% aesthetic ratio. It is well documented that implant volumes in excess of 400 cc tend to be associated with greater complication rates and this remains true in both augmentation as well as mastopexy augmentation (▶Fig. 29.3).

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


