25 Decision Making in Mastopexy Augmentation
Summary
Mastopexy augmentation is one of the most difficult and contentious procedures in cosmetic breast surgery. This chapter provides an overview of the decision-making process for the procedure.
Key Teaching Points
Mastopexy augmentation is used when ptosis occurs with either hypomastia or involutional atrophy.
Augmentation should always be performed before the mastopexy component of the procedure.
Smaller implants are preferred over larger devices as the patients have already demonstrated poor support.
Wide skin undermining should be avoided.
25.1 Introduction
Mastopexy augmentation is the process of augmenting breast volume coupled with elevation of the breast mound and nipple to emulate a more youthful breast appearance. Augmentation is most commonly performed using breast implants but can also be achieved with fat grafting. Elevation of the breast mound requires one of a host of mastopexy techniques. Coupled together, this procedure has achieved notoriety for being a somewhat risky enterprise by some surgeons, despite considerable evidence attesting to its safety when properly performed. It is, however, complicated by the combination of decision-making algorithms for both breast augmentation as well as mastopexy.
25.2 Patient Assessment
When counseling a patient presenting with an interest in mastopexy augmentation, it is imperative that a careful history be taken.
What are the patient’s desires and what goal is she seeking? Many patients who need mastopexy augmentation present initially requesting augmentation alone, and failure to perform the often-indicated mastopexy will result in a poor outcome.
Similarly, many patients presenting primarily for breast augmentation but who are assessed as needing mastopexy as well will express concern regarding the scarring associated with mastopexy, something that they were frequently not expecting.
The fact that this patient population tends to have poor elasticity, hence the need for an additional mastopexy in the first instance, places them at risk for subsequent stretching leading to recurrent ptosis and they should be warned that additional tightening of the skin envelope may be required downstream.
Breast tissue quality is often relatively poor with thin, stretched skin, and significant glandular atrophy leaving little padding over an implant.
These features add to the difficulty of achieving outstanding aesthetic results in this patient population. A very frank discussion should be had with these women to highlight the problems inherent in its execution.
25.3 Examination
25.3.1 Chest Morphology
The chest wall should be evaluated for length, width, and symmetry.
Patients with scoliosis frequently have asymmetrical anterior chest walls resulting in a need for asymmetric implant size and/or shapes.
The chest should be evaluated for pectus deformities:
Excavatum creating a tendency for the implants to want to fall in medially.
Carinatum will tend to push implants laterally.
Pearl
These patients should also be approached with caution as their pectoral muscles may be tight and intercostal muscles are often thin and easily penetrated during a subpectoral dissection. I often perform subfascial approaches in pectus patients so as to leave the intercostal muscle complex undisturbed.
The medial origins of pectoralis major should be determined. Laterally based origins predispose the patient to poor cleavage formation and the appearance of wide-spaced breasts. I prefer the subfascial approach in such cases, but great care should be taken to preserve medial perforators in order to reduce the risk of breast necrosis (▶Fig. 25.1).

25.4 Breast Examination
Breast dimensions can be measured with calipers and pinch thickness evaluated. This can aid in determining the appropriate implant base diameter for a given soft tissue envelope. I personally do not rely on base diameter measurements that much as three-dimensional (3D) imaging tends to result in patients selecting larger implant volumes than I had predicted on clinical grounds. Measurements do at least provide a starting point for the discussion regarding ultimate implant size, particularly when 3D imaging is not available.
The consistency of breast parenchyma is important when assessing soft tissue cover over an implant. Many patients with ptosis have significant involutional atrophy resulting in “stringy” glandular tissue with little fatty support. Further, the consistency of fat in some patients is soft and easily compressible while others have firmer, well-supported fat, which tends to create a “perkier” ultimate result. The thinner, less adipose breasts tend to need more implant support and more aggressive skin tightening procedures than those patients with better-supported breast tissue (▶Fig. 25.2).
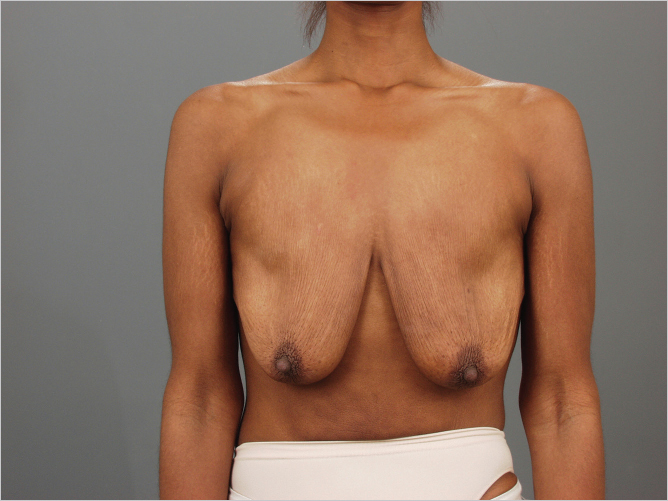
This is particularly true of thin, fit, multiparous women or massive weight loss patients, the latter being among the most difficult mastopexy augmentation patients to treat.
Obviously, any palpable breast masses or thickening should be evaluated carefully to exclude neoplasia.
25.5 Measurements
The important measurements in mastopexy augmentation patients include the following:
Nipple notch.
Inframammary fold–nipple distance.
Internipple distance.
Base diameter.
Medial and lateral pinch thickness.
Upper pole pinch thickness.
Areolar diameter.
Nipple length.
Any mastopexy procedure should take careful note of areolar diameter. Many such patients require areolar reduction as an integral part of their mastopexy. In patients with a large diameter, areolar reduction will result in the final nipple–areolar complex (NAC) having to travel a greater distance in a cephalad direction to meet the uppermost skin markings which in turn can create unwanted tension at closure. This should be taken into account when planning the procedure.
Pearl
It is imperative that the augmentation be performed first before committing to skin excision in order to minimize unwanted tension on suture lines.
25.6 Assessing Breast Shape
Malucci has characterized the features of the so-called “ideal” breast shape with the 45:55% ratio of upper to lower pole, respectively. This represents the ideal breast aesthetic in most of the Western world with the caveat that many American women favor more upper pole fullness than their European and South American counterparts. The significance for surgeons is that these variations in preference may determine what shape of implant is required for a given breast shape. This is further compounded by how much tissue is available to move superiorly to provide upper pole fill. A massive weight loss patient with near absent breast fat may require an implant profile with fuller upper pole fill than a younger woman with more normal breast fat quality.
Upper pole deficiency can be corrected well with an anatomical profile implant, particularly when additional lower pole fullness is desired. Conversely, when a patient desires the more rounded upper pole sought after by many American women, she may be better suited to a round high-profile implant. Similarly, narrow-chested patients require a narrower base implant and may be suited to moderate-to-high–profile devices while a broad-breasted women will require a wider base diameter to achieve a natural appearance. Maintenance of normal breast balance relative to chest diameter and overall body habitus is key to a successful, aesthetically pleasing outcome.
It should be borne in mind that the mastopexy technique selected will have significant impact on the ultimate breast shape achieved. A vertical mastopexy will narrow the breast diameter creating more coning of the breast while the Wise pattern techniques often preserve a wider base. Periareolar techniques tend to flatten the front of the breast resulting in a “pancaked” flat-fronted appearance with loss of central projection (▶Fig. 25.3).

Related posts:
 26 Periareolar Mastopexy Augmentation
26 Periareolar Mastopexy Augmentation
 29 Prevention and Management of Complications in Mastopexy Augmentation
29 Prevention and Management of Complications in Mastopexy Augmentation
 28 The Wise Pattern Mastopexy Augmentation
28 The Wise Pattern Mastopexy Augmentation
 27 Vertical Mastopexy Augmentation
27 Vertical Mastopexy Augmentation
 31 Vertical Superior Pedicle Breast Reduction (Modified Lassus Technique)
31 Vertical Superior Pedicle Breast Reduction (Modified Lassus Technique)
 54 Prevention and Management of Complications in DIEP Flap Reconstruction
54 Prevention and Management of Complications in DIEP Flap Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


