26 Correction of the Breast-Conserving Therapy Deformity Using Local Flaps
Local flaps are often the procedure of choice for the correction of breast-conserving therapy (BCT) deformities. Because these defects are irradiated and tend to have both a skin and volume component, 1 nonirradiated, vascularized tissue is typically transferred to provide bulk and coverage. The secondary correction of these deformities using local flaps became popular in the 1990s because of the dissatisfaction with aesthetic results following breast preservation and radiotherapy. 2 – 4 Although these patients often choose BCT to minimize the amount of surgery and preserve their breasts, they often require more extensive procedures to correct the deformity if one develops. Local flaps remains an excellent option for correcting BCT deformities after radiotherapy.
Advantages of Using Local Flaps
Timing
Reconstruction is best performed before radiotherapy; however, there are some advantages to performing delayed autologous tissue reconstruction a few years after the completion of radiotherapy. The main advantages are that the margin status has been determined, and the potential for compromised margins and the loss of a reconstructive option (that is, a flap) is less likely. 5 Another advantage of delayed reconstruction is that the patient has had several years of cancer surveillance and a documented disease-free status; however, she is not completely without risk of local recurrence.
Technique
The use of autologous tissue offers several advantages. It provides well-vascularized flaps consisting of muscle and fat for volume and skin for coverage when necessary. These flaps often assist with fluid reabsorption and wound healing within an irradiated and often compromised field. Numerous options are available for local flaps that are outside of the irradiated field, including the latissimus dorsi myocutaneous flap, chest wall perforator flaps, and abdominal flaps.
Disadvantages of Using Local Flaps
Timing
Delayed reconstruction of BCT deformities requires an additional surgical procedure that is often extensive, with more recovery time than the original resection. In addition, the breast tissue has significant scarring and radiation-induced changes that include fibrosis, edema, and compromised wound-healing ability.
Technique
The disadvantages of using autologous tissue techniques include the potential for donor-site morbidity, further flap-related complications, and local recurrence. In addition, a local reconstructive option will have to be used should completion mastectomy and reconstruction be necessary.
Classification of BCT Deformities
Box 26-1 Classification of Breast Deformity After Conservative Surgery and Radiotherapy
BCT deformities have a spectrum of severity, depending on the amount and type of tissue resected, the location of the defect, and the local effects of radiation at the wound site. 6 Numerous classification systems have been designed to correlate the deformity type with treatment options. In a recent review of all BCT deformities using the complexity-based, multitiered Fitoussi classification, 1 83% of all grade IV deformities required a myocutaneous reconstruction. 7
Indications for Flap Reconstruction
Numerous options are available for reconstructing BCT deformities, including fat grafting, parenchymal remodeling, implants, a local breast flap, and distant flaps. Most reconstructive surgeons prefer to use autologous tissues to correct these deformities, 3 because they tend to be more reliable and appropriately address the problem. The surgeon must critically examine breast deformities and determine what tissues are absent or injured. Although skin is often not removed as part of a partial mastectomy, there is invariably a relative skin loss that requires correction.
Patient Example
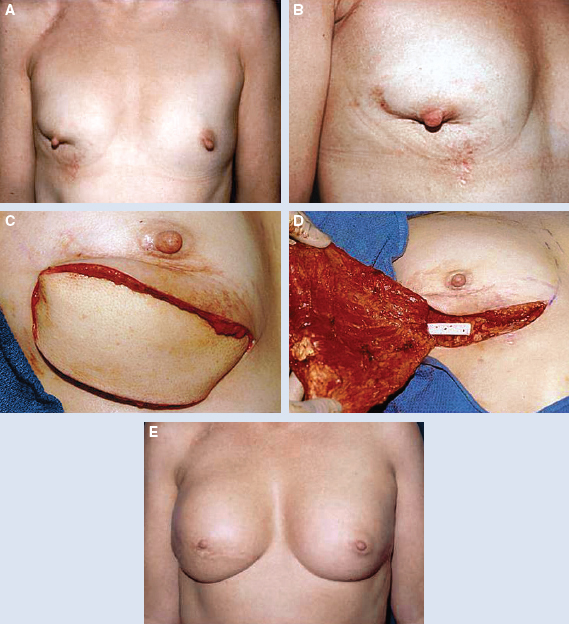
This patient presented with a retracted nipple-areola complex (NAC) 2 years after a lumpectomy and radiotherapy. Radiation changes to the skin included local hypopigmentation and telangiectasia (A and B). These changes necessitated a wide excision with release of the nipple-areola complex and resection of the damaged skin (C). A latissimus dorsi flap with a large cutaneous island was used to reconstruct the lower pole defect (D). Subpectoral implants were placed for symmetry. The size and shape are maintained 4 years after the flap transfer (E).
A thorough evaluation of the skin quality, including texture and surface abnormalities, helps determine the flap requirements. A contracted scar often distorts the breast contour and nipple position, requiring release and replacement with vascularized (nonirradiated) tissue. Once the tethered skin is released, the resultant defect and soft tissue requirement are often greater than anticipated. This possibility needs to be considered in the planning phase.
Breasts with significant skin envelope fibrosis and significant radiation changes always require flap reconstruction, regardless of the location of the defect. In addition to skin and contour analysis, breast symmetry should be assessed for volume differences, which will indicate the need for additional bulk with the flap. Most defects require skin and volume.
Every patient who has undergone BCT has a parenchymal deficit and requires volume augmentation in addition to skin coverage. Occasionally, volume is required without the need for skin coverage.
Unfavorable defects in almost any breast location can be reconstructed with local flaps. Larger medial defects often require options other than the latissimus dorsi flap. The main indication for correcting any BCT deformity is patient dissatisfaction with the cosmetic result after BCT.
Timing of Reconstruction
Unfortunately, the effects of radiation damage to the breast persist and need to be considered when planning reconstruction. During the reconstruction, it is critical to understand ongoing changes and anticipate future ones to optimize the aesthetic outcome. Appropriate preoperative cancer screening is crucial before reconstruction.
Following BCT, the breast undergoes early alternating changes of edema and retraction, so it is important to wait long enough after radiotherapy to schedule reconstruction to ensure that the breast’s shape and cosmesis have stabilized. A delay of 1 to 3 years is recommended.
Related posts:
 28 Local Perforator Flaps in Oncoplastic Breast-Conserving Surgery: The Nottingham Experience
28 Local Perforator Flaps in Oncoplastic Breast-Conserving Surgery: The Nottingham Experience
 27 Perforator Flap Reconstruction of Breast-Conserving Therapy Deformities
27 Perforator Flap Reconstruction of Breast-Conserving Therapy Deformities
 29 Breast Lumpectomy Reconstruction With External Vacuum Expansion and Autologous Fat Grafting
29 Breast Lumpectomy Reconstruction With External Vacuum Expansion and Autologous Fat Grafting
 31 Can Implants Correct a Breast-Conserving Therapy Deformity?
31 Can Implants Correct a Breast-Conserving Therapy Deformity?
 30 Fat Grafting in the Breast-Conserving Therapy Deformity
30 Fat Grafting in the Breast-Conserving Therapy Deformity
 24 Classification and Analysis of the Breast-Conserving Therapy Deformity
24 Classification and Analysis of the Breast-Conserving Therapy Deformity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


