24 The Wise Pattern Mastopexy
Summary
This chapter summarizes the approach to more aggressive skin resection applicable to severe ptosis, which is not readily treated with short scar vertical techniques. The Wise pattern procedure utilizes a longer transverse scar in the inframammary fold, allowing for shortening of the vertical scar length to restore balance to the overall breast shape.
Key Teaching Points
Wise’s pattern mastopexy is essential in cases of severe ptosis.
The horizontal skin excision allows shortening of the vertical scar length to restore balance to the breast shape and correct pseudoptosis of the gland.
Scarring is more extensive.
There is a greater risk of scar hypertrophy laterally and medially in the IMF.
Delayed wound healing at the inverted-T juncture can be problematic if closure tension is too high.
Skin flaps should not be widely undermined so as to avoid necrosis.
24.1 Introduction
Horizontal scar mastopexies involve varying degrees of skin excision based on the severity of the degree of ptosis. The more severe the ptosis, the more extensive is the skin resection required to achieve satisfactory correction of the underlying ptosis.
Technical Pearl
Insertion of an implant will reduce the amount of skin resection necessary, and will augment the upper pole, which is so often deficient in this group of patients.
Two basic groups of technique are available for severely ptotic patients:
Short horizontal scar approach—Marchac technique.
Wise pattern traditional approach with longer horizontal scar.
For patients with grade 2 bordering on grade 3 ptosis, a short horizontal scar Marchac-style mastopexy may suffice. In patients with severe grade 3 ptosis, a standard Wise pattern design is much safer with more predictable correction of the ptosis.
24.2 Vertical Scar Technique and Short Horizontal Incision (Marchac)
This variation of the vertical scar technique described previously is used primarily for moderate ptosis, when the distance from the areola to the inframammary crease is longer than 7 to 8 cm. The longer the vertical component of the final result, the more out of balance the breast appears, transgressing Malucci’s 45:55 principle. The addition of a short horizontal skin ellipse is preferable to the alternative of extending the vertical ellipse below the inframammary crease. The amount of transverse skin excision depends on the amount of excess skin and skin elasticity. Ideally, the vertical limb length should be shortened to 6 to 7 cm at most.
This 39-year-old patient was concerned about breast hypoplasia and involution, upper pole flattening, a low nipple, pseudoptosis, and breast asymmetry. She requested nipple–areolar elevation and a breast augmentation. The nipple–areolae were elevated with a periareolar incision and a vertical incision. The 240-cc smooth-surface implants were placed in a subpectoral position above and a subglandular position below (▶Fig. 24.1).
Surgical Plan
(See the Surgical Plan for Vertical Mastopexy)
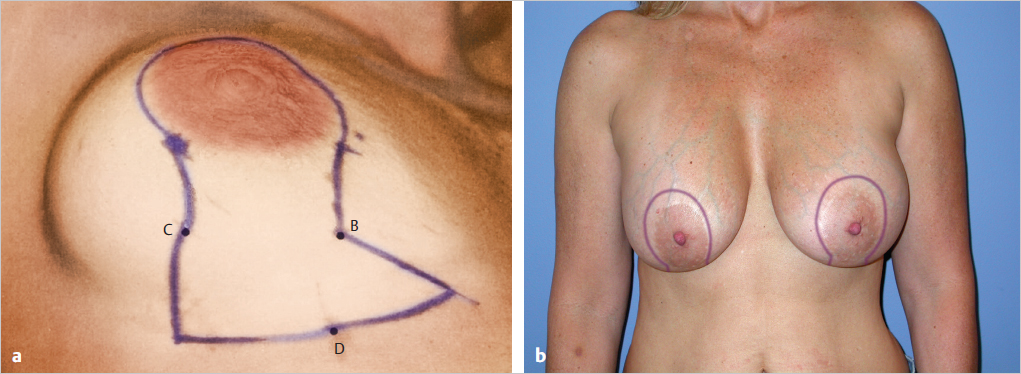
Preoperative markings for a short horizontal ellipse to reduce the length of the scar and prevent excess folding of skin.
Planning for a vertical limb approximately 6 to 7 cm from the areola to the inframammary fold (IMF) to ensure a short vertical limb and placement of the horizontal scar in the IMF.
The use of a more traditional inverted-T scar for the excision of a wider, lower skin ellipse to improve the breast elevation.
24.2.1 Markings and Technique
Accurate nipple placement is the first consideration, because it is used to determine the location and extent of the vertical and horizontal ellipses. The amount of skin resection of the lower pole and the size and position of the implant also influence these incisions. For this reason, I usually make the final decisions regarding the skin excision after these steps of the procedure are completed (▶Fig. 24.1).
Technical Pearl
If augmentation is planned, it should always be performed first before committing to any skin excision whatsoever.
The proposed nipple position is determined (see Vertical Mastopexy without Augmentation). If the distance from the postoperative lower areolar margin will exceed 7 to 8 cm, then some plan for a lower short horizontal ellipse is made. Markings for the ellipse are conservative; the final skin excision is performed after implant placement and parenchymal adjustment.
This 39-year-old patient was concerned about breast hypoplasia and involution, upper pole flattening, a low nipple, pseudoptosis, and breast asymmetry. She requested nipple–areolar elevation and a breast augmentation. The nipple–areolae were elevated with a periareolar incision and a vertical incision. The 240-cc implants were placed in a subpectoral position above and a subglandular position below.
The horizontal component was reduced by excising the vertical portion first and then excising only the excess horizontal skin. Preoperative markings for the standard inverted-T pattern can result in a closure that is too tight and leaves long horizontal scars. Problems related to excessive skin excision can be reduced by tailoring and excising the excess skin to fit the new breast mound.
The incision is made about the proposed new areolar circumference, and the skin of the vertical ellipse is excised. The dissection proceeds around the lower pole of the breast parenchyma. A subpectoral dissection is made for placement of the implant beneath the pectoralis major muscle above and in the subglandular position below. After the 325-cc implant is placed, the margins of the skin excision are approximated, and the nipple–areola is moved to the new position. The distance from the lower areolar margin to the inframammary fold (IMF) is determined. A point about 6 to 8 cm below the areolar margin, depending on the implant diameter and breast width, is selected and marked as the IMF. The skin between these two points is the amount to be removed. It is marked out as the shortest possible ellipse, excised, and closed with layered absorbable sutures (▶Fig. 24.2).
24.2.2 Results
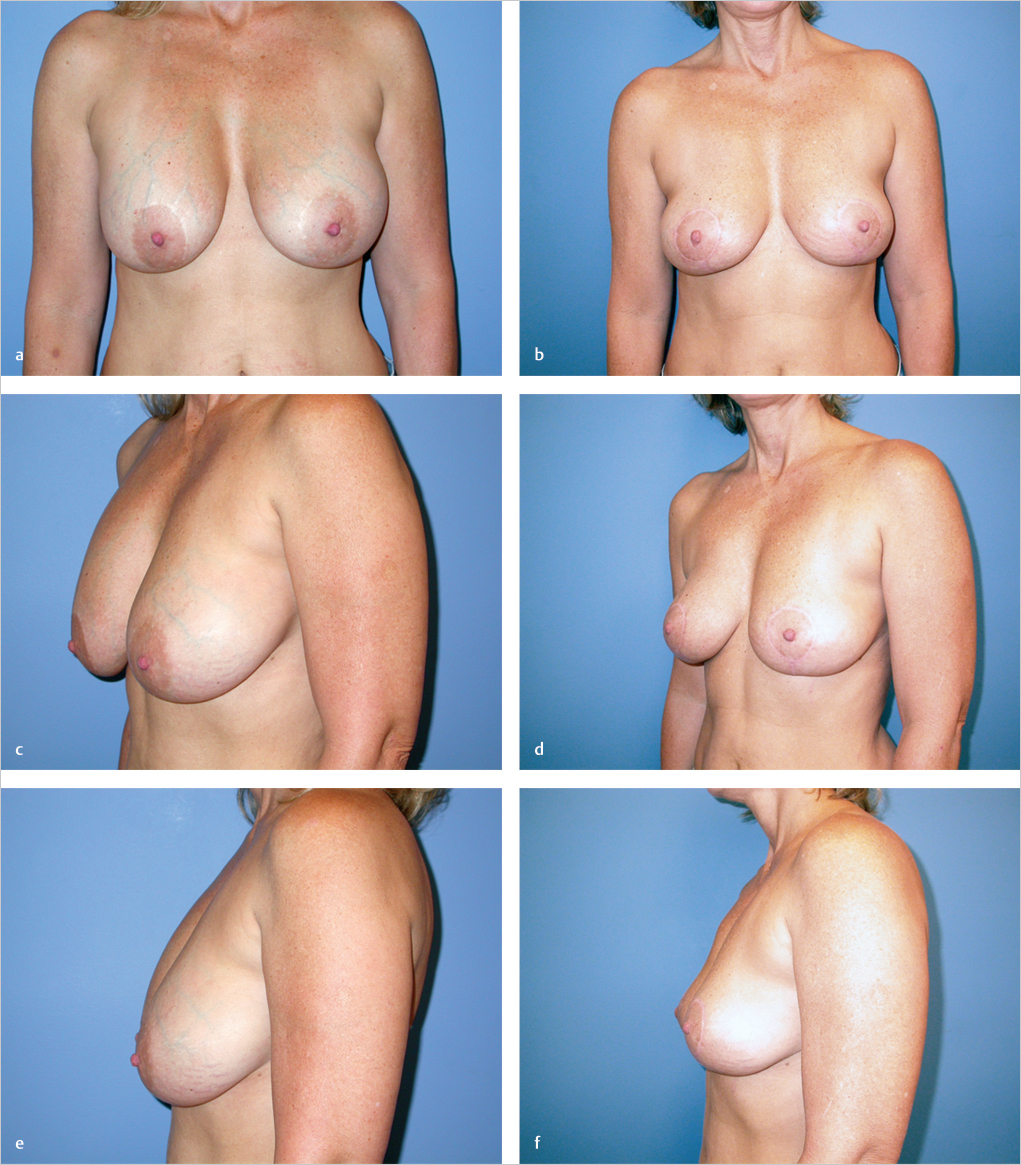
This 41-year-old woman had bilateral subglandular augmentation with periareolar mastopexy 10 years ago. She had always been dissatisfied with the heaviness of her augmented breasts and was troubled by unattractive venous distension within the skin of the breasts. This engorged appearance never resolved with time. She requested explantation with further mastopexy to improve her breast shape and reduce their weight. The implants were removed, creating more ptosis intraoperatively as expected. A vertical mastopexy was performed, but I thought that she would benefit from a transverse skin resection, and a short horizontal scar was incorporated in this procedure. The patient is shown 2 years after the procedure, with acceptable breast shape, retention of ptosis correction, and dramatic reduction in venous engorgement of her breasts. She was delighted with the outcome, despite the decreased breast volume (▶Fig. 24.3).
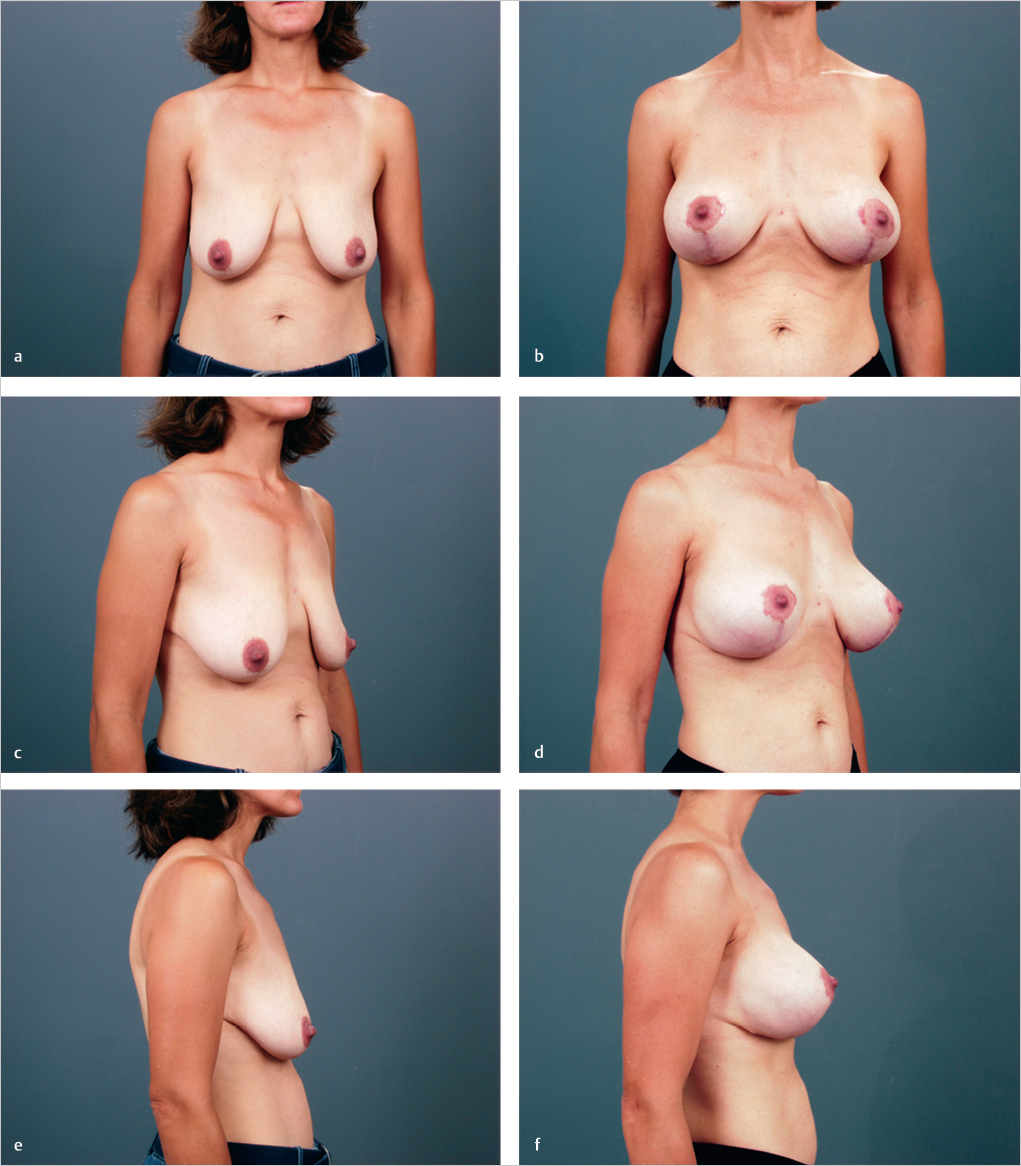
This 45-year-old woman developed involutional volume loss after lactation and very significant breast ptosis that was worse on the right than the left. The nipple-to-notch measurements were 29 cm on the left and 30 cm on the right. She requested breast augmentation with mastopexy. A subpectoral augmentation was performed with 275-cc implants, followed by an overlying vertical mastopexy. When the patient was placed in the erect position intraoperatively, it appeared that she could easily develop a tendency for pseudoptosis of the implant, because her dermis was extremely thin. A short horizontal scar was incorporated into the mastopexy. Instead of discarding the horizontal skin island, it was deepithelialized and sutured beneath the implant to the underlying rib periosteum to provide internal support for the implant. Two years after surgery, she has reasonable retention of shape and nipple–areolar diameter, although her scars, particularly in the periareolar area, have remained rather pink with several small areas of periareolar scar hypertrophy. She reports that her nipple sensation has returned to normal (▶Fig. 24.4).
24.3 Wise (Inverted-T) Technique with (or without) Implant Placement
The inverted-T technique is used when there is major ptosis, the lower breast area is relatively full, and the nipple–areola requires a relatively long transposition. The technique is similar to superior pedicle breast reduction, except that little or no breast tissue is removed other than that removed for final shaping of the lower pole. Patients suitable for this approach often have an acceptable breast volume but with marked flattening in the upper breast region and ptosis of most of the breast parenchyma below the inframammary crease.
Technical Pearl
To determine whether a patient’s breast volume is satisfactory for this approach, the breast is manually elevated to the position the patient desires. If she still wants upper breast fullness, a breast implant will be necessary. An implant is frequently required.
Simply tightening the skin over the supporting breast will not accomplish upper pole fullness. If the breast volume is appropriate, I resect some of the ptotic lower breast parenchyma below the inframammary crease and replace this volume with a breast implant to give upper breast fullness and some central breast projection. It is rare for me to perform a Wise pattern mastopexy without concomitant breast augmentation.
Surgical Plan
(See the Surgical Plan for Vertical Mastopexy)
Adjustment of preoperative markings to accommodate 1 to 2 cm of additional vertical and inferior tissue resection to prevent tight closure.
Long-term correction based on the lower tissue pole resection.
Transfer of the areola on the superior breast parenchyma and excision of additional skin after implant placement and before the final closure.
Augmentation as indicated.
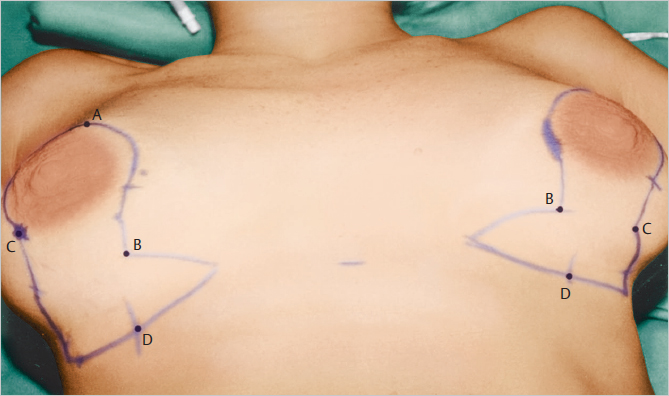
24.3.1 Markings and Technique
Preoperative markings are similar to those for reduction mammaplasty.
Technical Pearl
Because an implant will be used, I do not mark as much skin for excision. I prefer to excise additional skin after the implant has been placed so as not to create excessive tension leading to skin necrosis.
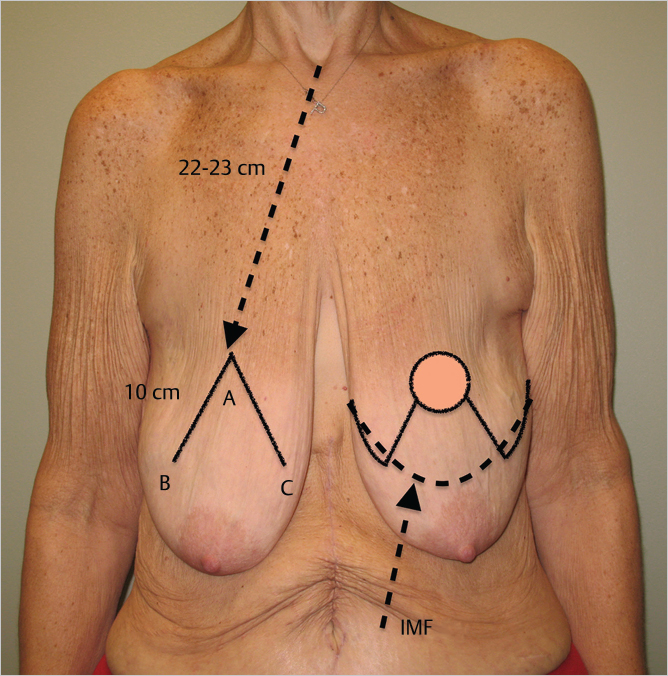
Markings are made with the patient in the sitting position. The point A for the top of the areola is about 1 to 2 cm above the inframammary crease, and between 22 and 23 cm from the sternal notch depending on the breast volume. The vertical limbs extend inferolaterally from the 7 and 5 o’clock positions on the lower areolar marking for a distance of 10 cm to points B and C. From these lowermost tips the lateral and medial wings of the horizontal excision can be marked, but I usually do not incise and commit to the horizontal excision until the augmentation is complete. This central inverted V is designed beginning at the point of the areola apex and extending around the nipple–areola to a point approximately 10 cm below the top of the future areola position. This is basically a conservative skin ellipse; additional skin can be removed at the end of the procedure. The markings are made in the inframammary crease. The breast is displaced, first laterally and then medially, to connect the lines that mark the future inframammary crease. The new diameter of the nipple–areolar circle is drawn, usually 38 to 42 mm. The incision is made around the nipple–areola, and the upper skin within the V markings is deepithelialized (▶Fig. 24.5).
If augmentation is to be performed, it is done through a vertical midline incision in the lower pole of the breast directly below the 6 o’clock position of the areola. A dual-plane approach is planned.
The inframammary crease incision and the future inframammary crease incisions are made. Any ptotic breast tissue below the inframammary crease is excised and the amount recorded. Dissection is continued along the depths of the breast and upward to the pectoralis major muscle, and a dual plane pocket is created above (▶Fig. 24.6).
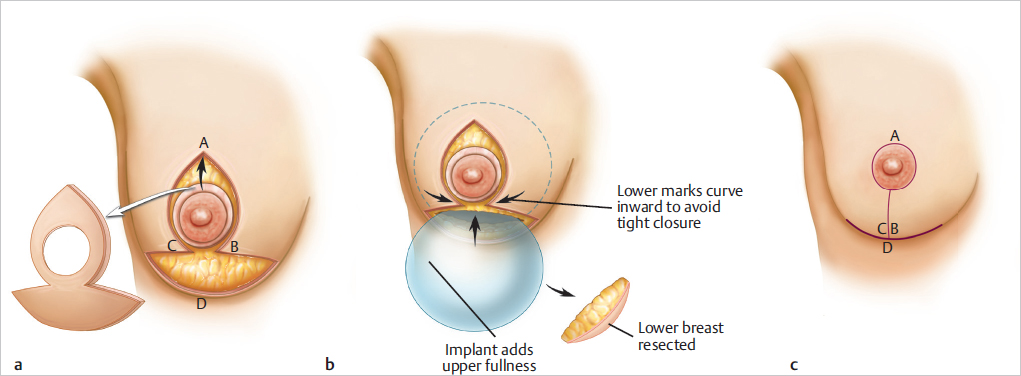
This pocket is expanded medially to accommodate the breast implant when the patient wants significant upper breast fullness. I like to use a temporary sizer to determine the appropriate volume replacement. The implant is selected to provide appropriate fullness in the central breast and upper breast regions. Wound closure is accomplished in layers, and the lower breast parenchyma is sutured to the inframammary crease to give good implant coverage. An incision is made around the periphery of the V to permit mobilization of the nipple–areola to its new position. The wound is closed laterally and medially toward the center of the T. Any excess skin along the vertical limb is excised. The incision is closed from the point of the T upward to create a vertical limb length of about 5 to 6 cm. The nipple–areola is cut out as a circle with a diameter a few millimeters smaller to avoid a tight areolar closure and a widened scar. The incision is closed with layers of absorbable intracuticular sutures. A periareolar Gore-Tex cartwheel suture is inserted to prevent areolar dilation if an implant has been used.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


