22 Nasal Reconstruction
Summary
While minor, and frequently nonoperative, injuries to the pediatric nose are common, major injuries are relatively rare. Acquired defects can occur as early as infancy due to pressure-related necrosis of the septum, columella, or ala during nasal oxygen administration as in continuous positive airway pressure (CPAP). The more common cause of nasal defects occur during childhood as a result of animal bites and burns. All such injuries are important from a psychological and developmental standpoint. The importance of self-image plays into the psychosocial development of the pediatric patient, and reconstructive efforts should be made in some attempt before the child starts school, approximately by 6 years of age. Defects of the pediatric nose are especially challenging due to the complex anatomy of the nasal structures and the need to grow with the rest of the face. The relative presence or absence of the various nasal components (external skin, cartilaginous or bony support, or internal lining) should be noted and addressed as appropriate.
22.1 Introduction
Given the causes for major pediatric nasal reconstruction are relatively rare, the importance of the nose, from both a psychological and developmental perspective, mandates that they be done with great care. As evidenced by the existence of punitive rhinotomy, described in historical documents since times even before the Code of Hammurabi, undeniably the nose carries a psychosocial importance that supersedes almost any other aspect of the human body. Additionally, from a developmental perspective, the nose is considered one of the growth centers of the face, responsible for some of the development of the midface during childhood as well. Subsequently, defects of the pediatric nose from both congenital and acquired etiologies take on a heightened level of complexity, not only due to the complex anatomy of the nose, but also due to the overall impact that nasal development will have on both psychosocial development and the ultimate development of the face. Furthermore, reconstruction of the pediatric nose carries with it special concerns including whether the reconstruction will grow with the face, how the reconstruction could alter remaining facial development, and if or how future donor sites should be preserved should a future revision be necessary.
22.2 Embryology
At minimum, a cursory understanding of the embryologic development of the nose and face is important when considering reconstruction of nasal anomalies, given these malformations are by definition the result of aberrant embryogenesis and an ability to assess what nasal components or subunits are absent or malformed will subsequently lead to an understanding as to what will need to be replaced during the course of reconstruction.
As an overview, the pediatric face begins to take shape during weeks 5 to 10 with the formation, fusion, and differentiation of five mesenchymal swellings or prominences: two mandibular, two maxillary, and the unpaired frontonasal. The latter will ultimately be responsible for forming the face above the external nares, including the forehead, interorbital region, and the majority of the external nasal structures, while the maxillary prominences will comprise the oral opening to the external nares and the mandibular prominences will fuse to create structures inferior to the oral opening (Fig. 22‑1).
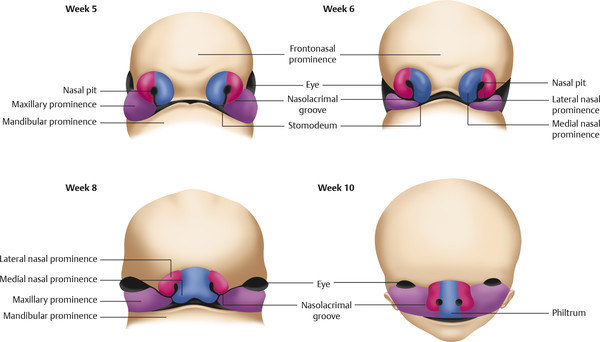
Initially, development of the nose begins with formation of the nasal placode from localized thickening in the superficial ectoderm of the inferior portion of the frontonasal prominence, immediately above the nasolacrimal groove between the frontonasal and the maxillary prominences. Sensory neurons in the placode differentiate to form olfactory neurons, while thickening of the mesenchyme at the periphery of the placode elevates the ectoderm above the placode to produce nasal pits at week 5. The outer areas of these pits will form the medial and lateral nasal prominences, from the inferior portion of the frontonasal process. The medial nasal prominences ultimately fuse together to form the median nasal prominence at week 8 (leading to the creation of the nasal dorsum) and will also fuse inferiorly with the lateralized maxillary prominences to form the central and lateral portions of the upper jaw, including the philtrum, nasal septum, and the primary palate. The lateral nasal prominences fuse with the more cephalad aspect of the maxillary prominences to form the nasal alae as well as lateral portions of the nose. The maxillary prominences also will go on to form the secondary palate, an example of the interconnectedness of nasal and palatal formation explaining why cleft palate malformations are inherently linked to nasal deformations as well.
22.3 Development
After birth, the nose continues to grow and change with the facial profile throughout adolescence. The infant nose is noted to have less frontal projection with a shorter dorsum, larger nasolabial angle, and rounder nares. The main support of the infant nose is the dorsal septal and upper lateral cartilages, which are considered an extension of anterior cranial base. This cartilaginous septum is considered to be a part of two nasal growth centers, the sphenospinal zone and the sphenodorsal zone, both of which affect the growth of not only the nose itself, but also the surrounding midface. The sphenodorsal zone is described as being responsible for growth in the length and height of the dorsum, while the sphenospinal zone is responsible for sagittal growth, as well as outgrowth of the maxilla. Because of the presence of these growth zones, loss of septal cartilage in infancy and childhood can lead to various acquired facial syndromes involving not only the nose, but also the maxilla and the orbit. Furthermore, surgery on the nose that disrupts these growth centers may have similar and predictable deleterious effects. Nasal growth appears to continue until early adulthood with specific windows of accelerated growth. The two most significant nasal growth spurts occur in the first 2 years of life and during puberty. The end of the period of growth was found to be at 12 to 16 years in girls and 15 to 18 years in boys.
22.4 Diagnosis
Defects of the external framework of the nose are generally obvious on inspection. They can arise from congenital and acquired causes. Congenital defects occur generally as a result of failed or incomplete fusion of the mesenchymal prominences discussed previously. For example, failed development of the frontonasal prominence results in the characteristic deformities seen in frontonasal dysplasia. Another class of congenital defects arises as the result of congenital growths such as benign hemangiomas (Fig. 22‑2), dermoid cysts, and nasal encephaloceles (Fig. 22‑3). A classification scheme developed by Losee et al separated nasal malformations into four broad classes. Type 1, comprising 62%, includes defects arising from hypoplasia or atrophy and agenesis syndromes ranging from whole arhinia to individual subunits including nostril stenosis (Fig. 22‑4), nasal hypoplasia, choanal atresia, and craniofacial syndromes. Type 2 defects (1%) are the result of hyperplasia and duplication exemplified by proboscis lateralis. Atypical clefts comprise type 3 and arise from failure of fusion of medial or lateral nasal prominences and the surrounding maxillary prominence and include the Tessier 0, 1, 2, and 3 clefts as well as their cranial extensions 11, 12, 13, and 14 (Fig. 22‑5). Neoplasm and vascular anomalies are included in type 4 nasal defects (20%). Examples of benign lesions include hairy nevus, glioma, pilomatrixoma, neurofibroma, and nasal dermoid (12.4%), as well as benign vascular lesions such as hemangiomas.




Acquired defects of the nose can occur throughout infancy and childhood and include both iatrogenic and hospital-acquired conditions, such as pressure-related necrosis of the septum, columella, or ala during nasal oxygen administration as in CPAP (continuous positive airway pressure). The most common cause of nasal defects during childhood is traumatic, resulting from animal (generally dog) bites and burns.
Further diagnostic maneuvers may include one or more imaging modalities to better elucidate the nature of the deformity. If there is a question of depth or involvement of surrounding tissues, a computed tomography (CT) scan or magnetic resonance imaging (MRI) may be indicated. CT scanning will highlight the surrounding bony structures and determine if there is potential involvement of deeper structures. MRI will better elucidate the soft tissues in and around the nose.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


