23 Facial Paralysis
Summary
The management of pediatric facial palsy begins with the accurate multidisciplinary assessment of the deficit and acute problems, the cause and associated problems, the likelihood of spontaneous recovery and the psychological and social impact on the child and their family. After the management of acute issues (which are uncommon), once there is a decision to operate, an assessment is made of the surgical options. Which one is used depends on the exact deficit, but in general in the pediatric group the problem is the inability to smile. Our preferred option is a two-stage procedure in which the first stage is a cross-face nerve graft and the second stage a free gracilis transfer. This is gone through in detail with the family, and the decision to proceed is made together with them. The outcomes are generally good, with the vast majority of patients who have received the two-stage procedure achieving improved facial symmetry, developing an ability to smile spontaneously, and also very satisfactory results for those receiving free gracilis transfers innervated by the motor nerve to masseter and the complication and revision rates are relatively low.
In terms of the future, recent evidence from the rat model suggests that “super-charging” the nerve graft with a sensory nerve at the time of grafting can improve nerve regeneration. Brief periods of electrical stimulation of a proximal nerve stump can also enhance nerve regeneration. Finally there are also potential pharmacological avenues that may improve outcomes in nerve regeneration, such as geldanamycin and FK-506.
23.1 Introduction
The muscles of facial expression are perhaps the most obvious outward, involuntary expression of our internal emotional state. Impairment of its actions is not life-threatening, but will alter not only the appearance of the face at rest and in motion, but also, possibly, ocular and oral continence. Interestingly, these latter two are often not a significant issue in the pediatric population. The problem that most often brings the pediatric patient to the facial palsy clinic is in fact their inability to smile. Simply not being able to smile spontaneously at the appropriate time during a social interaction has a significant impact on the individual’s psychological state and potentially also on the perception of others about the individual.
Pediatric facial palsy is relatively rare, and as with many pediatric conditions can be categorized into the congenital and acquired. Although facial palsy present at birth has an incidence of 2.1/1,000 in newborns, most are acquired and associated with birth trauma such as forceps use, and the incidence of actual congenital cases is closer to 0.24/1,000—around 90% of birth-injury-associated palsies show complete recovery. Facial palsy acquired after birth, while less common than in adults, is usually associated with an infective process and typically presents with an acute-onset facial paralysis, the most common reasons being Bell’s palsy, acute otitis media, and Lyme disease, and has an annual incidence of 6.6/100,000. The management of the patient should be within a multidisciplinary environment that incudes ear, nose, and throat surgery, rehabilitation therapy services, psychosocial support, and a pediatric medical assessment.
23.2 Comparison with the Adult Population
The etiology of the disorder. In congenital or developmental facial palsy, it is not possible to re-neurotize using the ipsilateral facial nerve. Furthermore, there may be no useful muscle units, and if dynamic reconstruction is required, the use of a functional muscle transfer is mandated. Also, in cases of bilateral facial nerve palsy even the contralateral facial nerve may not be available to use as donors. Importantly, facial palsy apparent at birth is not necessarily a “development” problem, but may be secondary to birth trauma, for example, following the use of forceps.
Psychosocial. The ability of a child to be able to respond to a facial expression with their own (gestural coupling) is important for psychosocial development, and its loss may affect not just the perception of others about the child with facial paralysis, but also how the child understands others. On the other hand, patients who acquire facial palsy already have established social functioning. The psychosocial implications, therefore, of a facial palsy are potentially greater in the congenital than the generally older, acquired group.
Expectations. The adult population with facial paralysis tend to have a lower expectation of what must be achieved (primarily focused on functional issues) and are often keen for less involved procedures to achieve more simple results, whereas the opposite is the case for the younger population—often driven by parental desire for a child who can integrate “normally” with their peers.
Peripheral and central neural plasticity. Peripheral nerve healing in children is much more effective than in adults. Therefore, greater success can be expected in techniques for facial reanimation that depend upon it in children compared to adults. Furthermore, central plasticity is also better in the younger patient and is of particular merit in procedures in which a nerve other than the facial is used to innervate a reconstruction.
Co-morbidities. In the elderly adult group with, for example, malignant parotid tumors, anesthetic limitations and the likely prognosis may limit which procedures are appropriate. In the pediatric population, the facial palsy may be syndromic and reanimation must be coordinated with other treatments and may be affected by them. For example, in hemifacial microsomia, the final aesthetic outcome will also be very dependent upon the craniofacial reconstruction, or where a future maxillary osteotomy may be needed, a cross-facial nerve graft that could be injured by such a procedure may be contraindicated.
23.3 Anatomy of the Facial Nerve and Muscles of Facial Expression
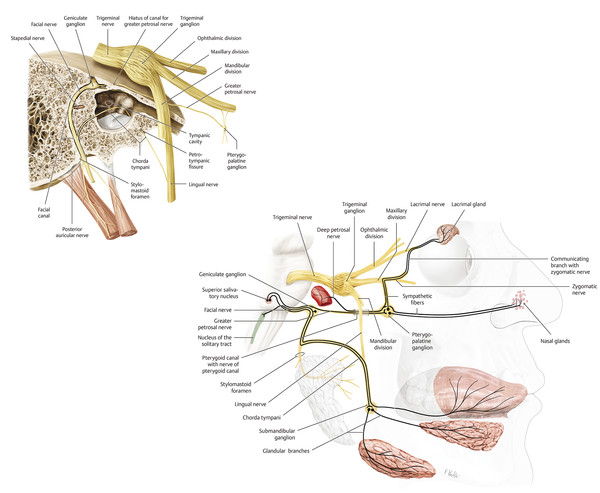
The first branches of the facial nerve once it leaves the stylomastoid foramen are the posterior auricular branches, which are motor to occipitalis, and branches to the stylohyoid and posterior belly of digastric. The nerve then has a short course between the foramen and the parotid gland through which it passes, separating it into deep and superficial lobes; despite this intimate relationship, the facial nerve provides no innervation to the parotid. As it passes through the gland, the nerve branches into the pes anserinus, and by the time it exits the parotid is classically said to do so in five major branches: zygomatic, temporal, buccal, marginal mandibular, and cervical (Fig. 23‑1). This is, however, an oversimplification and there are not only multiple branches, but also a significant degree of cross-innervation between branches.
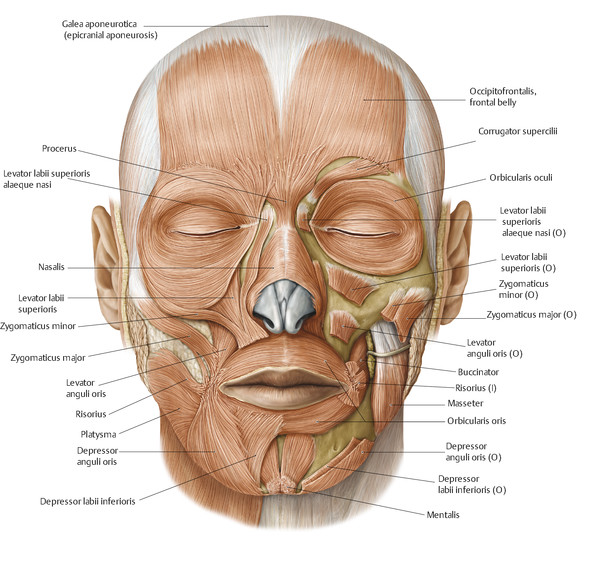
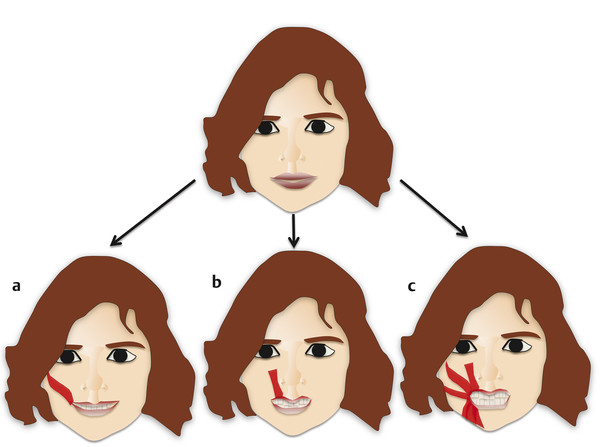
The nerve is deep to the superficial aponeurotic system (SMAS), and it supplies the muscles of facial expression. The muscles are layered into four levels, and the branches of the nerve lie deep to all but the deepest layer (which consists of the buccinator, mentalis, and levator anguli oris). The muscles may be divided roughly into thirds: an upper group (in the supraorbital and periorbital region), a midface group, and a lower face group. The upper group (frontalis, procerus, and corrugator supercilii) originate laterally and superiorly and insert into the glabellar and supraorbital area. They function to animate the eyes and periocular regions. With the exception of nasalis, the muscles of the midface and the lower face insert into the oral commissure and thus animate the lips (Fig. 23‑2). In 1973, Rubin described three basic types of smile (Fig. 23‑3). The first, the “Mona Lisa” smile, accounted for 67% of his subjects and was due to the dominant action of the zygomaticus muscles. The second, “canine smile”, accounted for 31% and was due to a greater dominance of the levator labii superioris. The third group was the rarest, the “full denture smile,” which accounted for just 2% of the study group and was felt to be due to roughly equal forces being applied to the lips from all the muscles inserting into them. We believe aiming for a line that mimics the zygomaticus muscles gives the best results.
At the nasolabial fold, the facial musculature integrates with the dermis. The consequence of this uniquely intimate relationship between the underlying muscle and the overlying integument is that relatively small movements have a significant effect on the overlying skin and soft tissues. Also, as a result, unlike in muscle transfers elsewhere, it is our experience that the insertion of the muscle should be to the dermis in order to effect the best results. Following denervation, the motor endplates at the neuromuscular junctions atrophy such that by 2 years following the loss of their nerve supply, they are not functionally re-neurotizable. Following facial nerve injury, therefore, this defines the window of opportunity available to re-innervate the muscles.
23.4 Diagnosis and Assessment
It is important to recognize that facial paralysis is not necessarily a diagnosis in itself, but often a sign or symptom of an underlying condition. The assessment of the child with a facial paralysis is aimed at the following:
Recognizing underlying or associated symptoms.
Evaluation of the nature of the paralysis and its effects (and particularly any acute functional problems).
Working out reconstructive goals.
Working out reconstructive options.
Assessment is performed in a multidisciplinary environment including the surgeon, therapy services, a pediatrician, and potentially other specialities as required, such as ear, nose, and throat surgery. A targeted history and examination is performed to elucidate the likely cause of the facial palsy and therefore the prognosis and possible other medical problems, as well as therapeutic options. A list of the possible causes of the facial palsy is given in Box 23.1. In the history, the pertinent points are whether the palsy has been present since birth (and if so the type of delivery) or whether it was acquired, its duration, whether it is bilateral or unilateral, whether it is static, improving, worsening, or episodic, and other symptoms such as strabismus (as may occur in Moebius syndrome). If the child is old enough, information on the function of other parts of the facial nerve is also useful, such as whether there is reduced lacrimation or if hearing and taste have been affected. Furthermore, questions regarding functional problems such as epiphora and ocular trauma, speech impairment, and problems with feeding should be enquired about. Finally any history that may be suggestive of a specific neoplastic lesion should be aggressively pursued. The physical examination should focus on working out the level of the facial nerve injury, the branches affected, and the severity of the effect on the brow, periorbital area, midface, and lower face (Fig. 23‑4, Fig. 23‑5). Particular attention is paid to whether the eyes are affected, whether eye closure is complete, and if not the quality of the protective Bell’s reflex, as the combination of an inadequate Bell’s reflex and poor lid closure exposure is potentially sight threatening due to the resultant corneal exposure, though, ocular problems in the pediatric group are rare compared to adults. Other points of note on physical examination include any evidence of hemifacial microsomia, the position of the cupid’s bow on attempted smile—in congenital cases this tends to be more centralized—the function of the muscles of mastication and tongue (given the motor nerve to masseter and the hypoglossal are potential donors), the vector of the unaffected lateral lip element on smiling, and a “gestalt” view of the face. In our experience, electrophysiology does not alter management. Imaging will rarely usefully visualize the facial nerve, but may be relevant to identify other potentially important pathologies such as space-occupying lesions. Through this process, one should be able to determine the following factors: Is this congenital or acquired? What are the deficits? What does the patient/parents feel are the problems relating to appearance? What is the chronicity of this palsy? What are the available donors? What are the goals?
Box 23.1 Summary of Conditions That May Cause Facial Paralysis
Extracranial
Traumatic
Facial lacerations
Blunt forces
Penetrating wounds
Mandible fractures
Logogenic injuries
Newborn paralysis
Neoplastic
Parotid tumors
Tumors of the external canal and middle ear
Facial nerve neuromas
Metastatic lesions
Congenital absence of facial musculature
Intratemporal
Traumatic
Fractures of petrous pyramid
Penetrating injuries
Larogenic injuries
Neoplastic
Glomus tumors
Cholesteatoma
Facial neuromas
Squamous cell carcinomas
Rhabdomyoma
Arachnoidal cysts
Metastatic
Infectious
Herpes zoster oticus
Acute otitis media
Malignant otitis externa
Idiopathic
Bell palsy
Melkersson–Rosenthal syndrome
Congenital osteoporosis
Intracranial
Iatrogenic injury
Neoplastic: benign, malignant, primary, metastatic
Congenital
Absence of motor units
Syndromic
Hemifacial macrosomia (unilateral)
Mobius syndrome (bilateral)


Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


