2 Made to Match: The Essence of Breast Implant Selection
Summary
State-of-the-art breast implant–related surgery in primary augmentation, revision, or reconstruction requires the patient and plastic surgeon to navigate a number of critical decisions involving multiple factors. Implant selection and the patient education process this entails is the most critical and most challenging part of the surgical process. It involves evaluating patient expectations including reported bra cup size; optimally, three-dimensional imaging and simulation; and tissue-based planning, leading up to a sequence and algorithm assessing the specific indication for the procedure, the shape of the device, soft tissue assessment, implant softness and cohesivity, and, finally, implant style and size. This sequential, straightforward implant selection process is the essence of breast implant surgery and should assist the surgeon and patient who are navigating the important process of accurate patient assessment and implant selection so that they are truly Made to Match.
2.1 Introduction
Breast augmentation is a process, not simply a procedure. The key components as outlined by Adams 1 are comprehensive patient education and informed consent; tissue-based operative planning; refined surgical technique with rapid recovery; and detailed postoperative education. By far the most important of these processes are the first two: patient education and operative planning. In fact, if these first two critical steps are neglected, the surgeon may have performed a technically successful procedure, but the result may be deemed a failure by the patient.
With the advance of social media, the Internet, TV shows, and marketing as well as our profession itself, it is becoming increasingly difficult to meet a patient’s expectations, and it all begins with patient education. Surgeons have to make some very fundamental decisions when it comes to breast surgery and plastic surgery in general. Among the first is, “Am I looking to perform an augmentation to restore volume and shape and create a natural, proportional outcome based on the patient’s tissues, or not?” As we must decide whether we are going to place fat in the breast anywhere except the subcutaneous fatty plane, surgeons need to decide on how they will approach breast augmentation patients and whether they will use tissue-based planning techniques to determine implant selection, or not. This chapter will make several assumptions. The first is that the plastic surgeon interested in this chapter and approach uses current, tissue-based planning principles in selecting breast implants and educates patients to what this approach delivers. In general, it is advisable not to augment less than or greater than 1 cm of the patient’s breast base width. This principle creates a range of about 150–250 cc based on the implant’s projection. There is not one implant size or style that will work for any given patient. In fact, there are probably 10 to 15 implants that may work. The goal is to achieve a size that is best for the patient’s body to obtain a great outcome, but not so large or so small that it creates a complication, malposition, asymmetry, or suboptimal aesthetic result. Next, the patient’s cup size is standardized, and the patient is then shown three-dimensional (3D) imaging and simulation of the expected outcome. 2 If the surgeon’s recommendations and the patient’s desires do not align, the surgeon should try to educate the patient further or should consider avoiding operating on the patient.
Next, the surgeon should match the implant style and specific gel characteristics to each patient. There are hundreds of different styles of available implants on the market today. The benefit of having so many different implant styles, projections, shells, and gel cohesivities is that the surgeon can match the patient’s desires very well and even correct minor asymmetries. The challenge of having all of these possibilities is deciding which implant to use. One current implant manufacturer has over 900 implant options, and the product line continues to grow. 3 It is no wonder that what patients desire and demand as an acceptable outcome is becoming an increasingly difficult target to hit. The intent of this chapter is to arm the reader with the tools, techniques, and approaches to help simplify and navigate these core critical decisions that need to be made with the patient to achieve a successful outcome.
2.2 Bra Cup Sizing
A great deal has been written on patient education and informed consent, and one cannot overemphasize its critical importance in the entire education process. Trying to determine what a patient is looking to achieve and then educating that patient on what is or is not possible, cutting through all of the misinformation and myth, is a challenging task. Informed consent is not just a document. It is a process that walks the patient through the procedure in detail, including details of the procedure, options and alternatives to achieve the desired goal, the anticipated course and potential outcomes, and all potential complications in detail. One of the most difficult aspects of adequate breast augmentation informed consent is that there is no standard.
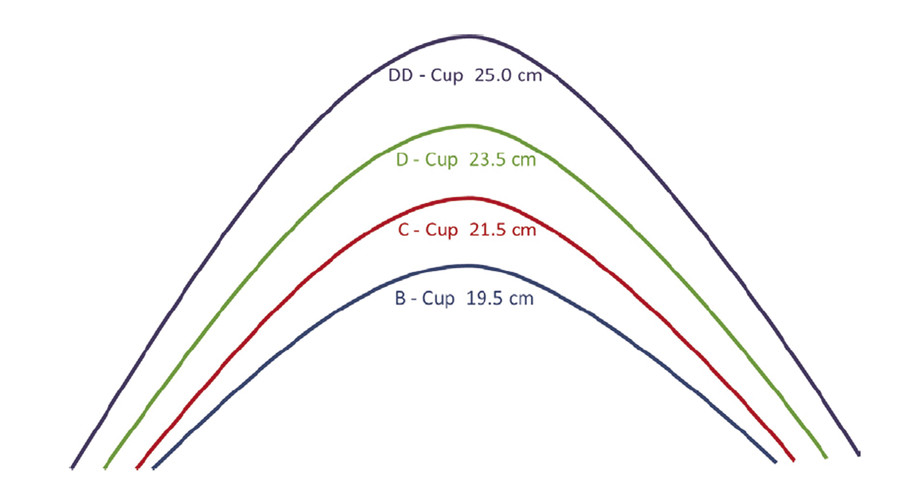
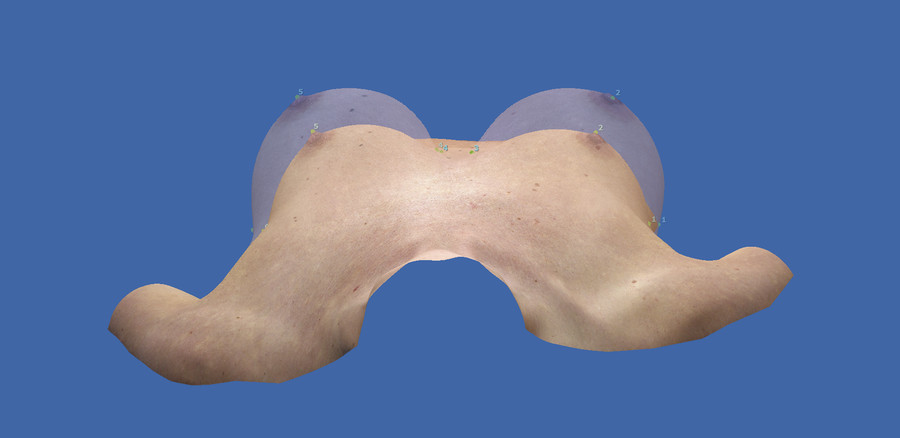
One of the challenges of standardizing outcomes is that bra sizing is variable and often times not reproducible. The author has developed a method to standardize breast cup size, and although still imperfect, it adds an incredible educational benefit for the patient–surgeon relationship and helps to create a standard starting point and endpoint with one simple measurement. 2 Most importantly, it enables the surgeon and the patient to begin the discussion on size. This, along with patient imaging, will enable the surgeon to come to an agreement on the range of outcomes for the patient. The bra cup can be standardized with one hemi-circumference measurement over the maximum apex of the breast, supporting the breast if it is ptotic. These measurements were determined from evaluation of over 6,000 patients and have been confirmed in over 3,000 more. Assessing and setting the bra cup measurement as a standard at the consult is an excellent educational tool that puts the surgeon and patient on the same starting page concerning size and allows for standardization for the outcome both as an objective measurement and visually when 3-D imaging and simulation are added. Once the bra cup size is established, adding approximately 200 cc raises the bra cup incrementally by one size. Bra cup sizing, along with the 3D imaging and simulation discussed in the following section, enable patients to visualize and experience their outcome before surgery. In the author’s experience, use of 3D imaging and simulation allows for the best visual for setting expectations and limiting the need for revisional surgery (Fig. 2‑1, Fig. 2‑2).
2.3 Three-Dimensional Imaging and Simulation
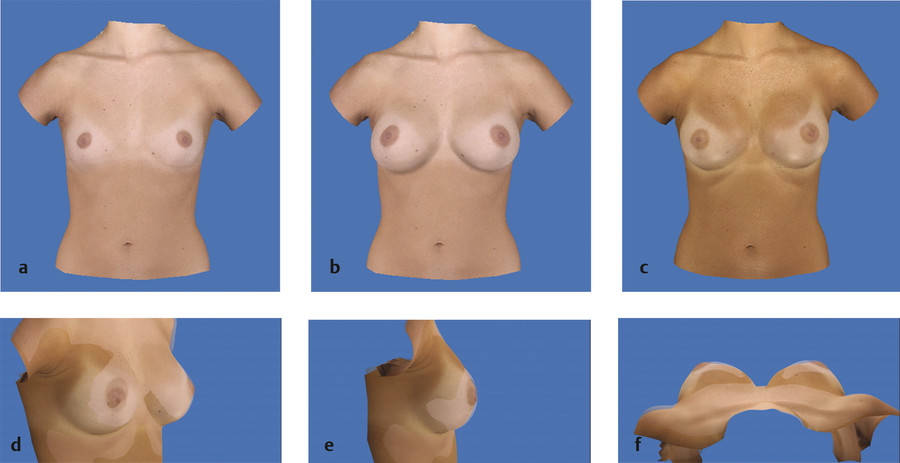
Along with the new cohesive implant options, imaging and simulation has been one of the most significant technical enhancements in the author’s practice in the past 10 years. It is not just a great marketing tool (although it certainly is that). It enables the patient to visualize the outcome. In addition, it is an incredible educational and planning tool, enabling the surgeon to determine volume and projection differences specifically from side to side. In striving for as much symmetry as possible, over 60% of the author’s patients receive implants that are asymmetric in volume or profile to achieve the best symmetry possible, because native breasts are often asymmetric to some degree. This technology is quite reliable; outcomes average less than 2% different from the simulation at 1 year (Fig. 2.3). 4 , 5 Mastopexy and augmentation–mastopexy procedures can also be simulated and used to walk patients visually through these procedures. The author is currently working on reduction and revision modules to simulate the removal of specific volumes or known implant volumes and subsequently adding volume back in or lifting the breast. 6
2.4 Implant Characteristics and Implant Selection
Implant selection using tissue-based planning principles has been very well documented, and the author currently uses a modification of the “High-Five” principles as outlined by Tebbetts and Adams. 7 , 8 The importance of using exam and measurements in selecting the implant range for each patient cannot be overemphasized. Each surgeon will need to decide how to help patients select a range of implants that match their breast and body. Key critical factors and assessments for general selection include the following:
Determine the patient’s breast base width (BBW). BBW is the actual breast width minus the soft tissue thickness (on average 1.5 cm). The actual breast width is measured as the transverse width from the medial to lateral inflection points of the breast, which represent the breast borders (Fig. 2‑4a). This BBW is critical and determines the overall range of implants. The author chooses implants with a diameter or width within 1 cm of the BBW.
Determine the sternal notch (SN)-to-nipple (N) (Fig. 2‑4b) and nipple-to–inframammary fold (IMF) distances. If the patient has a short SN-to-N distance, shorter-height and smaller-diameter implants are chosen, or alternatively, the IMF needs to be adjusted. N-to-IMF distance also affects implant diameter and height selection.
Determine breast type and compliance or elasticity. This helps to determine implant projection. This can be determined objectively or subjectively and, in general, can be classified as tight, average, or loose. The looser the skin envelope, the more projecting the implant needs to be, or, alternatively, mastopexy and skin reduction will be required to match the breast and implant volume (Box 2.1 and Fig. 2‑4c).

Fig. 2.4 (a) Breast base width (BBW), (b) SN-to-N distance, and (c) elasticity are the three critical assessments that need to be measured and help determine the implant range, height/diameter, and implant projection.
Box 2.1 Basic Principles of Implant Selection
Breast base width (BBW) helps determine implant range
Sternal notch–to-nipple (SN-to-N) distance and nipple-to-IMF determine implant height
Breast type and compliance-elasticity
Tight 0–2 cm, average 2–3cm, loose 3–4 cm
Help determine implant projection
Select implant and set IMF
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


