Abstract
This chapter discusses the salient considerations involved in determining the status and treatment of nevi (moles) and vascular malformations. The ABCDE criteria for screening nevi and determining possible malignancies are detailed. Guidelines for excision and biopsy are reviewed, and special consideration is given to giant congenital melanocytic nevi. Vascular malformations—including hemangioma, capillary, venous, lymphatic, and arteriovenous malformations—are also addressed. Postoperative care and outcome guidelines, including cosmetic considerations, are reviewed.
16 Nevi and Vascular Malformations
16.1 Goals and Objectives
Determine which nevi are suspicious and require excision or biopsy.
Understand the risks and treatment options for giant congenital pigmented nevi.
Appreciate the difference in presentation and typical course of the subtypes of vascular malformation.
Understand the treatment options available for each subtype.
16.2 Patient Presentation
Patients with nevi frequently present either on their own or referred by another physician (primary care or dermatologist). Frequently referred to colloquially in the United States as “moles,” the term “nevus” encompasses a broad range of different dermatologic findings. Typically, a nevus is a pigmented lesion on the skin which may or may not be raised and may or may not be hair bearing. Most are benign, but some need to be followed closely, biopsied or excised.
The standard benign pigmented nevus is called a melanocytic nevus. These are typically small, brown, or black lesions with smooth borders and even coloring. These lesions should be followed over time and any change in the characteristics of that lesion noted. There are risk factors which are determined based on the appearance of the lesion which can determine its likelihood to contain malignancy or progress to malignancy (melanoma). The acronym ABCDE has become a widely publicized tool for screening nevi for the possibility of malignancy.
A: Asymmetry—one half is not like the other half.
B: Border—an irregular, scalloped, or poorly defined border.
C: Color—is varied from one area to another; has shades of tan, brown or black; or is sometimes white, red, or blue.
D: Diameter—melanomas are usually greater than 6 mm (which is around the size of a pencil eraser) when diagnosed, but they can be smaller.
E: Evolving—a skin lesion that looks different from the rest or is changing in size, shape, or color. 1
Those lesions that meet one or more of the ABCDE criteria need further screening as that lesion may represent a dysplastic nevus or melanoma. A dysplastic nevus, or atypical nevus, is one that meets the clinical criteria above and may also have cellular atypia on histologic examination. These dysplastic nevi are usually benign and stable, but they are considered a risk for transformation to melanoma.
Dysplastic nevi may occur singularly, or as part of a larger disorder known as dysplastic nevus syndrome or familial atypical multiple mole melanoma syndrome (FAMMM). Patients with this condition have had multiple dysplastic nevi and at least one close relative who has had melanoma. These patients are at increased risk of melanoma and need to be followed every 6 months to yearly by a dermatologist for complete examination, total body photography, and dermoscopy. 2
Aside from the ABCDE lesions, there are other types of nevi which warrant consideration. A pigmented nevus which has a surrounding ring of hypopigmentation is called a halo nevus (Fig. 16‑1). The origins of these lesions is not understood, but it is surmised that an immune response was responsible for the involution of the pigmented area. 3 The appearance of a halo nevus should prompt an investigation looking for a primary melanoma of the skin or the eye as these have been associated with occult melanoma. Excision of these lesions is prompted by the clinical history of melanoma, atypical appearance of the lesion (ABCDE), or presence of multiple other atypical nevi. 4

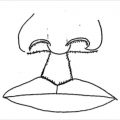
A salmon-colored nevus usually located on the head and neck area is called a nevus sebaceous (of Jadhasson; Fig. 16‑2). These lesions are present at birth and are flat. They typically become raised and develop a rough surface around puberty. Due to the risk for development of basal cell carcinoma, these lesions have typically been excised before puberty. However, studies have shown the incidence is less than 1%, so many are now excised only for cosmetic reasons. 5

Another type of nevus is a dome-shaped reddish or dark brown papule typically found on the head and neck and sometimes the thigh. Termed a Spitz nevus, it is common in children and rare in adults. Also known as “benign juvenile melanoma,” these nevi were once thought to be a form of childhood melanoma, but are now known to be benign nevi. These lesions usually require close observation or excision due to observational concern or confusion with melanoma. While there is no consensus, simple excision is usually adequate with 5-mm margins reserved for reexcision of pathologically atypical lesions. 6
When children are born with very large pigmented nevi (>20 cm in adults or predicted to reach 20 cm in diameter by adulthood. Or, 9 cm on an infant’s head or 6 cm on an infant’s body), they are termed “giant congenital melanocytic nevi.” 7 These lesions are often disfiguring and can be complicated by malignant melanoma and neurocutaneous melanosis. While these lesions are always present at birth, the extent of the lesion may not be known at birth due to variable degrees of pigmentation at birth which may increase over time. 4
Giant congenital melanocytic nevi most commonly occur on the trunk (sometimes called bathing trunk nevi) (Fig. 16‑3) followed by the extremities and then the head and neck. 8 Although at birth the lesions may be smooth and flat, over time the appearance and texture may change. They often develop prolific hair growth (1–2 years), a verrucous texture and variegation in color (around 10 years). 9 Most often there are also associated satellite lesions which can be located distant to the site of the main nevus. Children with leptomeningeal involvement sometimes present with seizures. 10

Typically, these giant lesions will expand in proportion to the body’s growth. The changes to the characteristics of these lesions need to be followed closely due to the risk of malignant degeneration to cutaneous melanoma or even noncutaneous melanoma (e.g., mucosa of gastrointestinal tract and retroperitoneum). The overall reported rate of malignant melanoma in these patients has ranged from 1.8 to 45%. 11 More recent studies have reported 2.8 to 8.5% with a lifetime risk of 6.3% and a relative risk of 17. Fifty percent of the malignancies arise during the first 3 years of life and 70% by puberty. 12
16.2.1 Preparation for Surgery
Most often the patients who will require surgery for nevi will be healthy. Age-related risk factors should be addressed as usual. In general, aside from any prior biopsy results, no further examination is warranted. The exception to this is in the children who present with a giant congenital melanocytic nevus and risk factors for neurocutaneous melanosis. These children have greater than 20 satellite nevi and congenital melanocytic nevi in a midline location over the trunk and calvaria. 8 , 13 This subgroup should be screened with MRI imaging of the brain and spinal cord between 4 and 6 months of age. Those with positive MRI imaging should be referred to neurosurgery, but the treatment of the cutaneous nevi need not be delayed. 12
16.3 Treatment
Pigmented lesions which meet the criteria for suspicion require biopsy or excision. Anesthesia and location for the surgical excision is dependent on the patient’s age and comorbidities, as well as the size and location of the lesion. Most young children will require a general anesthesia in an appropriate operating room setting with a pediatric anesthesia provider. Older children and adults with small to medium size nevi can be excised in an office or operating room with local anesthesia alone, local anesthesia with sedation, or general anesthesia. Very large lesions will probably necessitate general anesthesia. The author typically also utilizes 0.25% bupivacaine with epinephrine injected 7 or more minutes prior to incision to improve intraoperative hemostasis and to assist with postoperative pain control. Patients undergoing excision using local anesthesia alone or in conjunction with sedation will receive a 50:50 mixture of 0.25% bupivacaine with epinephrine and 1% lidocaine with epinephrine at least 7 minutes prior to incision.
Excision of these lesions needs to be full thickness. This is most commonly done as a full-thickness excision with 0 to 2 mm margins. A punch biopsy may be used if the punch incorporates the entire lesion. Very large lesions may be partially excised with a multiple full-thickness punch biopsies or incisional biopsies, but this introduces a significant amount of sampling error and should therefore be avoided. Shave biopsies of pigmented lesions are prohibited as this will destroy the crucial information of invasive depth of the lesion should the nevus turn out to be malignant. All excised tissue is sent for histologic examination. The results of this examination will dictate the need for any further excision.
For multiple reasons, giant congenital melanocytic nevi are treated in early childhood (as early as age 6 months). 14 The rational for surgical excision is to decrease the risk of malignant degeneration, aesthetic and psychosocial improvement, and to improve the ability to screen the lesions. While some have advocated the use of minimally invasive techniques to treat these lesions (curettage, dermabrasion, chemical peeling, lasers), none of these methods eliminates the risk of malignant degeneration (Fig. 16‑4). 12

Full-thickness excision of a giant congenital melanocytic nevus is most often recommended in the plastic surgery literature. Given the sheer size of these lesions, excision and reconstruction is often a challenge. Techniques include serial excision, tissue expansion, skin grafting, local and regional flaps, and free tissue transfer. A thorough discussion with the patient and/or family is clearly required detailing the risks and benefits for each of the procedures. Most often, if an excision can be accomplished in three or fewer stages, then serial excision with a minimum of 6-month intervals is recommended. 8 If four or more stages would be required, then tissue expansion becomes the preferred choice. Tissue expander techniques can be utilized to expand tissue for use as local, regional, or even free flaps. With the success of tissue expansion, the use of skin grafts, which often have suboptimal aesthetic results, has become much less common. 12
16.3.1 Postoperative Care
Postoperative care following excisional biopsy of atypical or other nevi is minimal. The wounds generally are small and heal quickly. The author most commonly utilizes dissolving suture and a skin adhesive as a dressing. This minimizes any necessary wound care and allows the patient a rapid return to normal bathing and other activities including swimming.
Following excision, patients need to be followed closely by a dermatologist. The interval at which they need to be seen will be determined by the diagnosis. Typically patients initially should be followed at 6-month intervals unless the nevus shows no atypia. Those with mild atypia are typically followed clinically. Those with moderate or severe atypia are often reexcised with 2 mm margins.
Postoperative care of the larger reconstructive endeavors for the giant congenital melanocytic nevi will depend on the procedure employed. These patients are frequently admitted after surgery for pain control and flap monitoring if necessary. Cases requiring placement of tissue expanders can be sent home with the majority of the expansion taking place as an outpatient—sometimes even at home by a responsible family member.
16.3.2 Outcomes
In general, complete excision of dysplastic nevi and other benign nevi will remove their malignant potential. Cosmetic outcomes will vary by the location and quality of the scar.
Oncological outcomes of treatment of giant congenital melanocytic nevi are related to the completeness of the excision and the degree of extracutaneous manifestation. Cosmetic outcomes are related to the size and location of the nevi, the techniques employed in reconstruction, and the quality of the scar.
16.4 Vascular Malformations
16.4.1 Patient Presentation
The term “vascular malformation” is steeped in controversy. It is really just a broad term which encompasses several very different lesions with very different presentations, different risks, and different treatment protocol.
Since there is no classic presentation for a “vascular malformation,” this term will be broken down into its individual components. A vascular malformation can be a hemangioma, a venous malformation, a lymphatic malformation, a capillary malformation, or an arteriovenous malformation. Several classification systems have been proposed. The most commonly used in the plastic surgery literature is that of Mulliken and Glowacki. 15
A hemangioma has proliferative endothelium, whereas the other types of vascular malformation have a stable endothelium. That means that a hemangioma is technically a type of tumor, while a vascular malformation is typically a benign lesion. The vascular malformations can be further broken down into fast flow (arteriovenous malformations) and slow flow (capillary malformations, venous malformations, lymphatic malformations). 16 , 17 There are also mixed lesions (lymphaticovenous malformations) which further complicate the discussion. This section will concentrate on the most common.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


