15 Zygomatic and zygomaticomaxillary complex (ZMC) fractures
INDICATIONS
Functional deficit resulting from coronoid impingement (limitation in ability to open mouth)
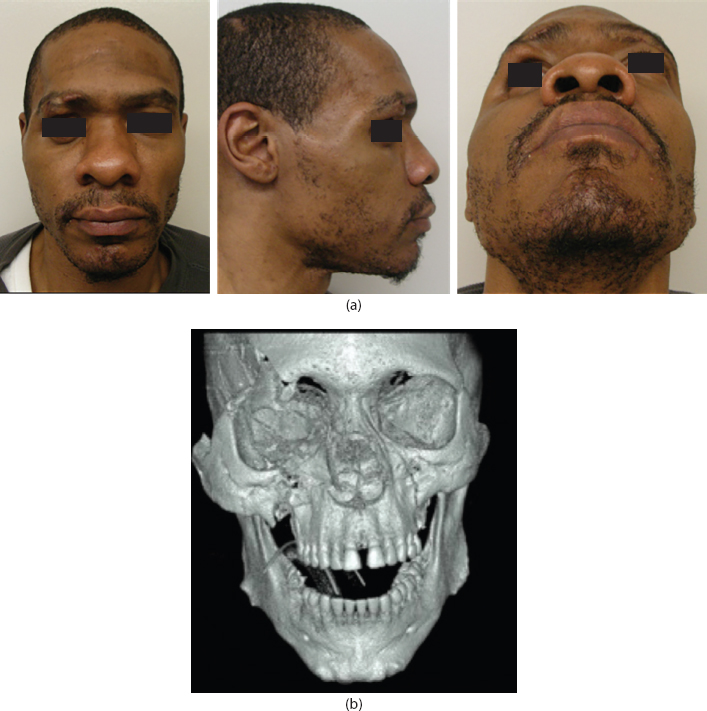
Treatment/prevention of contour deformity caused by skeletal malposition (malar projection, alteration in facial width, globe position) (Figure 15.1)
Basic soft tissue instruments (#15 blade, Adson forcep, Senn retractor, needle driver) Urethral sound or other long-handled blunt elevator Padded eye shield (for postoperative splint) |
Tray with soft tissue instruments sufficient for orbital approach and intraoral approaches to facial skeleton Carroll-Girard screw 28-gauge wire Plating system containing 1.5 and 2.0 plating options with low-profile plates for periorbital region Alloplastic implant or instruments to harvest autogenous bone (rib, calvarium) for orbital floor reconstruction |
INTRODUCTION
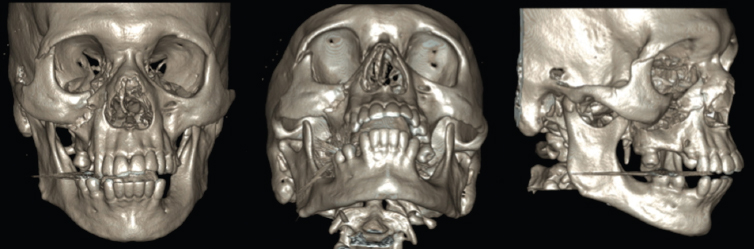
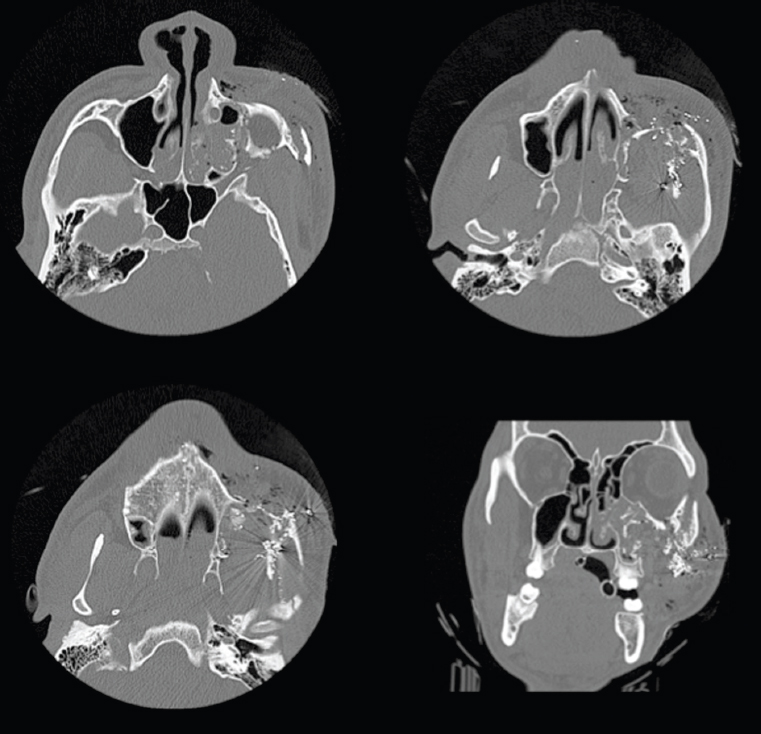
The zygoma is a spatially complex bone that articulates with the frontal bone, maxilla, temporal bone, and sphenoid. Zygomaticomaxillary complex (ZMC) fractures that occur with lower-velocity blunt impact often occur at these articulations. Spatially, they displace the ZMC with minimal comminution (Figure 15.2). Higher-velocity injuries (e.g., gunshot wounds) often cause comminution with more complex fracture patterns (Figure 15.3). By definition, given the anatomy of the zygoma, a ZMC fracture must affect the orbital floor or lateral orbital wall. Simultaneous reconstruction of the orbital floor is often indicated. ZMC fractures may cause deformity in facial width, orbital rim step-offs, cheek projection, and globe position. Medial displacement of the temporal process may cause trismus through impingement on the coronoid.
Direct impact to the lateral face may cause an isolated depressed zygomatic arch fracture. Significant displacement may result in loss of lateral facial width or trismus.
Treatment of zygoma fractures is generally: nonoperative (for nondisplaced fractures), reduction without fixation (for isolated zygomatic arch fractures) and exploration of the zygoma and articular processes with open reduction and internal fixation (ORIF). There remain several aspects of controversy in the latter treatment: the number of fracture sites that must be explored, sites requiring fixation for adequate stability, and ideal surgical incisions to achieve satisfactory exposure. This chapter presents our general approach, 1 representing our interpretation of the literature.
PREOPERATIVE MARKINGS
Reduction of depressed zygomatic arch fracture (Figure 15.4)
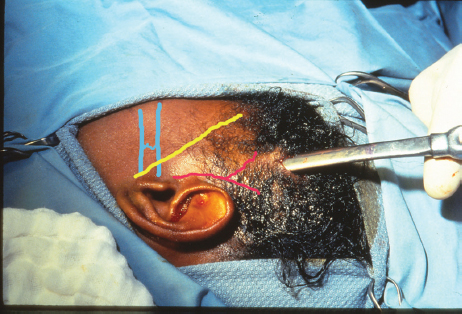
The position of the zygomatic arch and presumed fracture line is based on a computed tomographic (CT) scan and gentle palpation.
Course of temporal branch of facial nerve is determined.
Course of superficial temporal artery is determined (by palpation).
Avoiding items 2 and 3 above, a 1-cm long incision is designed within hair-bearing scalp. This generally originates superior and anterior to root of the helix of ear or just beyond.
Related posts:
 12 Cleft palate repair: The Furlow double-opposing Z-plasty, the Von Langenbeck palatoplasty, and the V-Y pushback palatoplasty
12 Cleft palate repair: The Furlow double-opposing Z-plasty, the Von Langenbeck palatoplasty, and the V-Y pushback palatoplasty
 14 Mandible fracture management
14 Mandible fracture management
 13 Orbital floor fracture
13 Orbital floor fracture
 11 Unilateral and bilateral cleft lip repair
11 Unilateral and bilateral cleft lip repair
 1 Skin grafting and dermal substitute placement
1 Skin grafting and dermal substitute placement
 16 Non-surgical facial rejuvenation with neuromodulators and dermal fillers
16 Non-surgical facial rejuvenation with neuromodulators and dermal fillers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


