12 Cleft palate repair: The Furlow double-opposing Z-plasty, the Von Langenbeck palatoplasty, and the V-Y pushback palatoplasty
INDICATIONS
INTRODUCTION
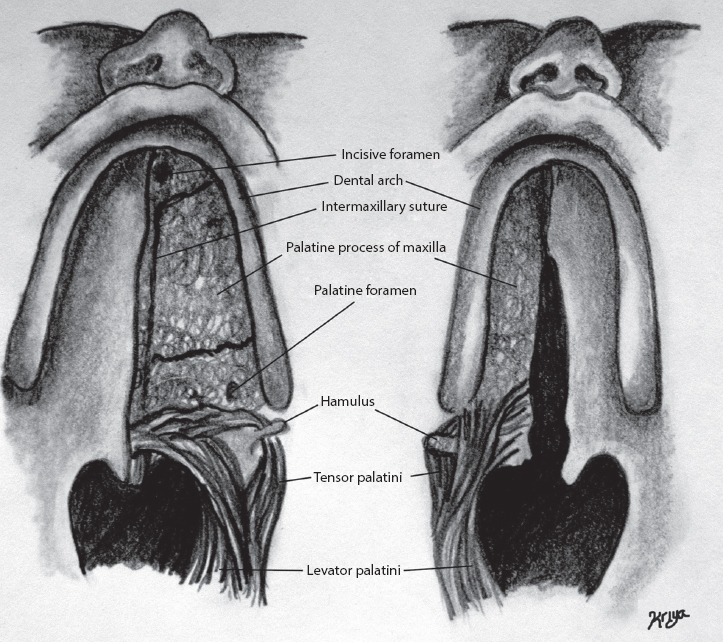
Worldwide, orofacial clefting, whether syndromic or non-syndromic, occurs in approximately 1 of every 500–700 live births. Clefting of the palate can occur with or without cleft lip. Isolated cleft palate, not associated with any other congenital malformations, occurs in 0.5 of 1000 births regardless of race. It is more frequently encountered in females (57% of isolated cleft palate patients). Conversely, clefting of the lip, whether isolated or associated with cleft palate, occurs with twice the frequency in males than in females. 2 Normal anatomy and cleft anatomy are shown in Figure 12.1.
Cleft palates are classified as primary if they are located anterior to the incisive foramen; when posterior, they are considered secondary. Primary and secondary cleft palates can be further subdivided into unilateral or bilateral (see Table 12.2 for Veau classification 3 , 4 ). Left unilateral cleft palate occurs twice as frequently as right-sided cleft palate. Unilateral cleft palate is nine times more common than bilateral cleft palate. 2
Regardless of cleft classification, surgery is necessary to create a free, intact palate with adequate mobility and functional musculature. The goal is to separate the oral and nasal cavities. Many studies advocate early surgery, usually from 6 to 18 months of age, although some surgeons have performed palatoplasties later in life, around the age of 2 to 3 years or even older. 5 Proponents of earlier surgery believe that there are improved speech outcomes and decreased incidence of hearing loss. However, others believe that it may lead to maxillary growth retardation 6 with associated dentofacial deformities. This may require later corrective orthognathic procedures.
Three widely utilized operative techniques are outlined in this chapter: the Furlow double-opposing Z-plasty, the Von Langenbeck palatoplasty, and the V-Y palatal pushback. The Furlow procedure aims to lengthen the soft palate and reorient the palatal muscles without elevating mucoperiosteal flaps from the hard palate. Some surgeons feel that this procedure can lengthen the palate by 20–30%. It has also been proposed that the double-opposing Z-plasty results in improved speech production 7 , 8 ; however, it may lead to increased fistula formation. 9 Some authors state that the Von Langenbeck procedure should be used to repair incomplete clefts of the secondary palate when there is no involvement of the lip or alveolus. 10 This technique reconstructs the cleft without associated palatal lengthening. As such, it may lead to a shortened soft palate with hypernasal speech. 5 V-Y pushback (Veau-Wardill-Kilner) is a variation of the Von Langenbeck procedure. It is frequently used for incomplete clefts involving the secondary palate. Some surgeons state it should be employed when there is decreased mobility of the soft palate or when lengthening of the palate is required. 3
OPERATIVE TECHNIQUE
Commonly used instruments are listed in Table 12.1. The first operative steps are similar for each procedure:
Measuring ruler Dingman retractor Small, medium, and large tongue blades Adson-Brown, Gerald, and Bayonet forceps Double-prong skin hooks Webster, Crile-Wood, and Castroviejo needle holders Curved iris, Metzenbaum, and Stevens tenotomy scissors Cottle periosteal elevator Kleinert Kutz periosteal elevator Obwegeser periosteal elevator Cleft palate raspatory and sharp hook Angled Beaver lamellar blades (60° bevel up) Mallet 2-mm osteotome 2-mm chisel Surgicel Nu-Knit |
The surgeon should be positioned at the head of the table.
Place a shoulder roll to hyperextend the patient’s neck.
Place the Dingman mouth gag.
Perform procedures with surgical loupes to enhance visualization.
Make the preoperative markings.
Infiltrate with 0.5% lidocaine and 1:200,000 epinephrine using a 23-gauge needle along the preoperative markings until the tissue blanches. Do not directly inject in the region of the greater palatine vascular pedicle. Always aspirate to ensure that there is no intravascular administration.
The Furlow double-opposing Z-plasty
PREOPERATIVE MARKINGS
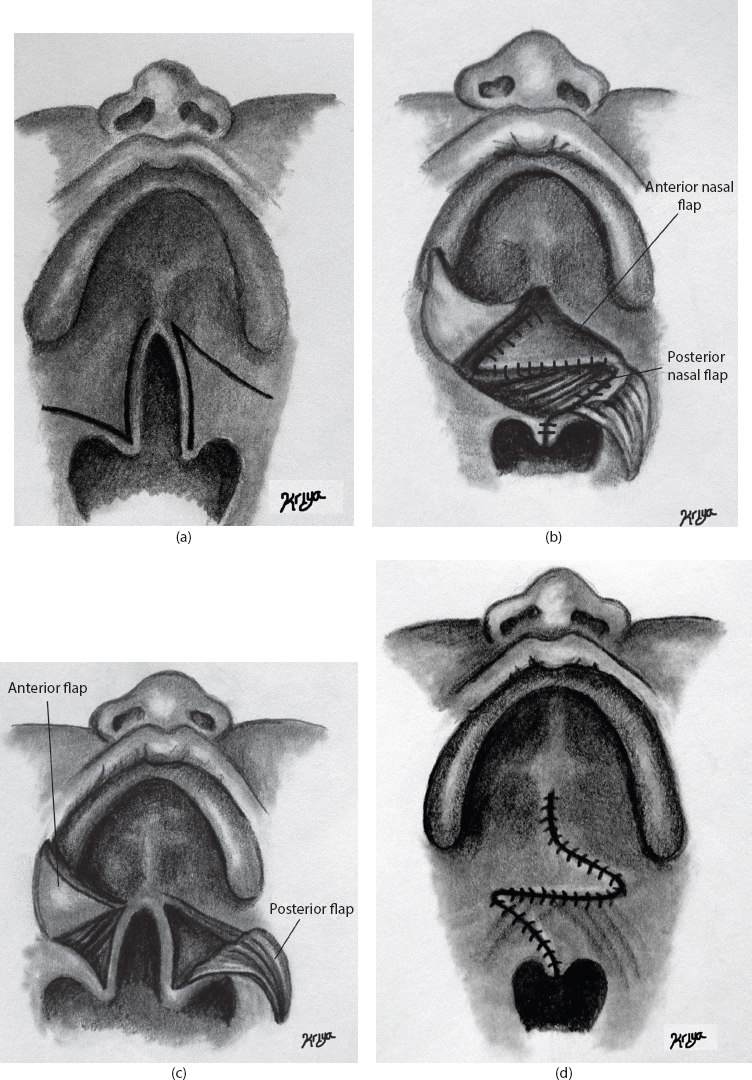
A Z marking should be made on the oral palatal surface with angles of approximately 60°. Lateral limbs of the Z should extend to the hamuli so that one of the lateral limbs lies along the hard palate’s posterior margin. Mark either side of the cleft margin to 4–5 mm before the tip of each hemiuvula (Figure 12.2a).
INTRAOPERATIVE DETAILS
A Z incision is made in the oral mucosa with angles of approximately 60°. Wider clefts will require more obtuse angles for adequate mobilization of flaps. 1
Lateral limbs of the Z on the oral mucosa should extend to the hamuli so that one of the lateral limbs lies along the posterior margin of the hard palate (Figure 12.2a).
Begin dissection by carefully incising the mucosal edges of the cleft with a #15 blade surgical scalpel so that there is a near equal amount of mucosa allocated to each side. Commonly, there is a distinct junction that exists between the nasal and oral mucosa at the most posterior portion of the soft palate cleft margin. 11
Extend the incision along the cleft margin anteriorly and elevate the mucoperiosteum of the hard palate, taking care not to damage this tissue at the cleft margin. This will be utilized for later closure.
Elevate the posterior oral flap by deepening the lateral incisions as well as the incisions along the cleft margin. This maneuver will also elevate the palatal muscle within the flap (Figure 12.2b).
Underlying nasal mucosa has a bluish appearance and must not be injured or torn during the dissection of the palatal muscles.
Use curved nasal scissors to carefully separate the palatal muscle from its bony insertion and from the nasal mucosa.
Reflect the flap and incise the palatal aponeurosis.
The myomucosal flap is now free to be placed across the cleft.
Elevate the base of the anterior oral mucosal flap and mobilize it from the area of the greater palatine foramen, taking great care not to lift the muscle with it.
Oral flaps are ready to be retracted to expose the nasal layer (Figure 12.2b).
Because the nasal Z-plasty is created in mirror image to the oral Z-plasty, its posterior flap, on the side of the palate where the oral flap contained only mucosa, should contain the muscular portion of the tensor-levator aponeurosis 11 (Figure 12.2c).
Cut the lateral limb of the posterior nasal Z-plasty along the hard palate margin, leaving 2 mm of nasal mucosa as an edge for sutures to be placed. This incision is important because it will free the palatal aponeurosis and will allow the posterior muscle flap to move across the cleft.
Incise the nasal mucosa and elevate the anterior nasal flap. When making the two lateral incisions of the nasal Z-plasty, extend each incision to the lip of the eustachian orifice.
The posterior nasal flap (containing nasal mucosa and muscle) is placed across the cleft posterolaterally and secured to the lateral recess in the palatopharyngeal tissue with an absorbable suture. The anterior nasal flap (containing only mucosa) is moved anteromedially and secured to the palatal shelf mucosa using another absorbable suture (i.e., 4-0 chromic) (Figure 12.2c).
Uvular tags are united with absorbable suture.
With the flaps transposed across the cleft, suture the anterior nasal mucosal and posterior nasal myomucosal flaps together (Figure 12.2c).
The oral myomucosal flap is positioned posterolaterally and sutured at the level of the hamulus, using either a 4-0 Monocryl® (Ethicon, Somerville, NJ) or Vicryl® (Ethicon) suture.
The oral mucosal flap is inset and sutured to the hard palate margin.
Place two 3-0 Vicryl sutures through the nasal and oral layers to secure the flaps.
Bring the hard palate mucoperiosteum into a horizontal plane and close with horizontal mattress sutures (Figure 12.2d).
Oral Z-plasty may require a back cut at the end of the lateral limbs, taking great caution not to injure the greater palatine vessels.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


