13 Orbital floor fracture
INDICATIONS
Three primary surgical indications for the repair of fractures of the orbital floor are:
Orbital floor fractures greater than 2 cm or >50% of surface area of the orbital floor
Enophthalmos >2 mm
Incarceration or entrapment of extraocular muscles
There are currently a number of surgical approaches to the orbital floor. Two of the most commonly used techniques are:
Pre-septal transconjunctival approach with or without canthotomy
Cutaneous approach
INTRODUCTION
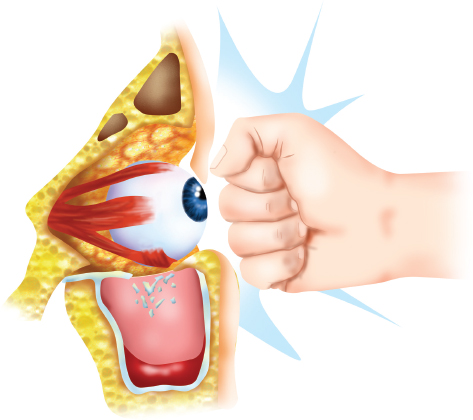
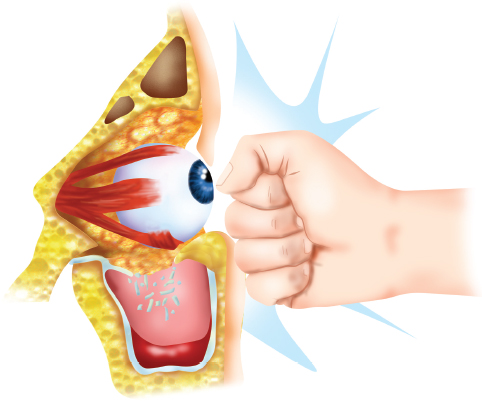
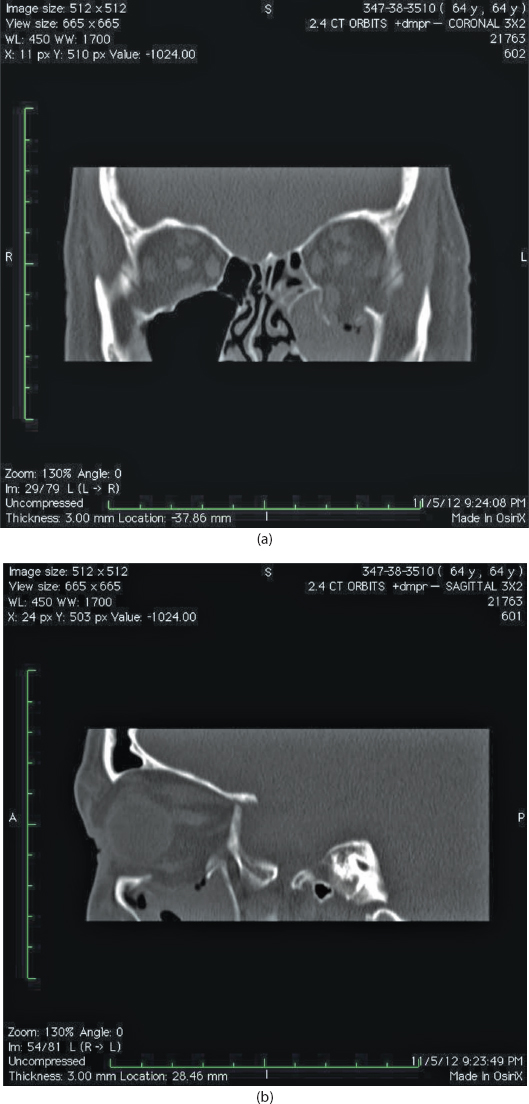
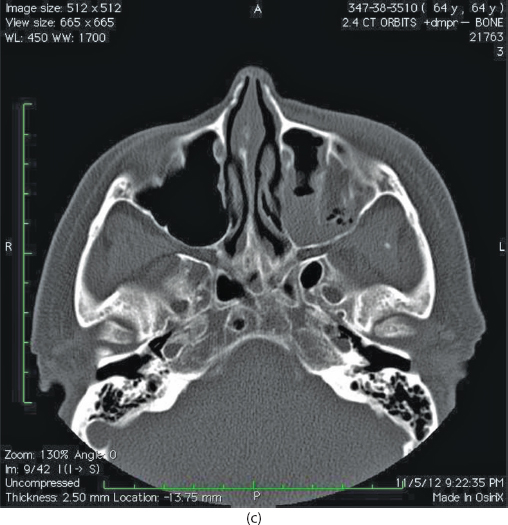
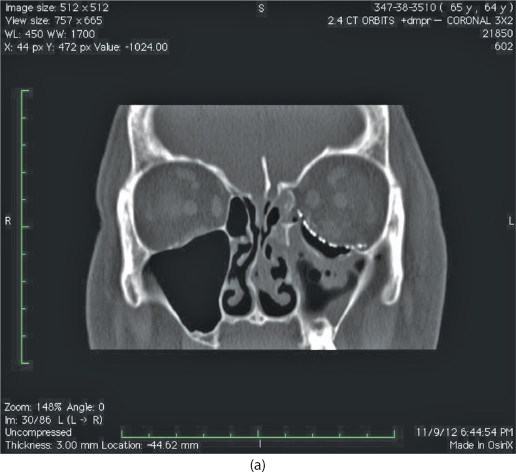
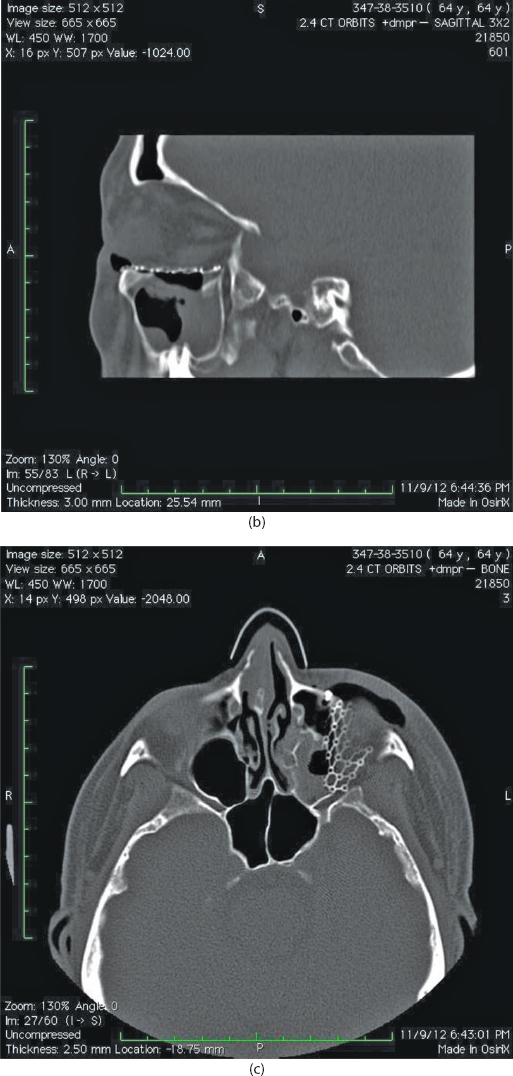
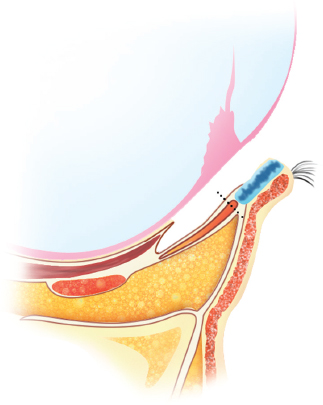
Isolated orbital floor fractures (blowouts) are often the result of impact injury to the globe resulting in a sudden increase in intraorbital hydraulic pressure. This kinetic energy is transmitted in an inferior and medial vector to the orbital floor (hydraulic theory) (Figure 13.1). Alternatively, the posterior transmission of a direct blow to the infraorbital rim causes buckling and resultant fracture of the orbital floor (buckling theory) (Figure 13.2). Fractures of the orbital floor can increase the volume of the orbit with resultant enophthalmos and hypoglobus. These can be highlighted on preoperative (Figure 13.3a–c) and postoperative (Figure 13.4a–c) computed tomographic (CT) scan imaging. In addition, the inferior rectus or periorbital soft tissue can become entrapped within the fracture line, resulting in restriction of extraocular eye movements. Table 13.1 indicates the special equipment used to surgically manage this injury.
0.5% topical ophthalmic tetracaine hydrochloride 1% lidocaine with 1:100,000 epinephrine 30-gauge needle Lubricating ophthalmic ointment Needle-tip electrocautery 5-0 nylon suture 6-0 fast-absorbing gut suture Desmarres retractor Small blunt-tip dissection scissor Cotton-tip applicators |
TRANSCONJUNCTIVAL APPROACH TO ORBITAL FLOOR FRACTURE REPAIR
Preoperative markings
A marking pen is used to make a surgical markings 2 mm inferior to the lower border of the tarsal plate (Figure 13.5).
The medial extent of the markings should be in line with the inferior punctum.
The lateral extent of the markings should be several millimeters medial to the lateral canthus.
Related posts:
 12 Cleft palate repair: The Furlow double-opposing Z-plasty, the Von Langenbeck palatoplasty, and the V-Y pushback palatoplasty
12 Cleft palate repair: The Furlow double-opposing Z-plasty, the Von Langenbeck palatoplasty, and the V-Y pushback palatoplasty
 14 Mandible fracture management
14 Mandible fracture management
 15 Zygomatic and zygomaticomaxillary complex (ZMC) fractures
15 Zygomatic and zygomaticomaxillary complex (ZMC) fractures
 11 Unilateral and bilateral cleft lip repair
11 Unilateral and bilateral cleft lip repair
 1 Skin grafting and dermal substitute placement
1 Skin grafting and dermal substitute placement
 16 Non-surgical facial rejuvenation with neuromodulators and dermal fillers
16 Non-surgical facial rejuvenation with neuromodulators and dermal fillers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


