14 Mandible fracture management
INDICATION
All displaced mandible fractures
INTRODUCTION
The treatment of mandibular fractures can be challenging due to the complexity of mandibular shape and the various sites at which fractures can occur. Although the vast majority of mandible fractures can be successfully treated by up to a 6-week period of maxillomandibular fixation, most contemporary management focuses on internal fixation of the fractures followed by immediate function. The focus of all surgery for these injuries should be on restoring the preinjury occlusion and establishing complete bone union. Table 14.1 indicates the equipment needed for these surgeries.
24- and 26-gauge wire Erich arch bars Electric or gas-powered drill system Mandibular plating system, including plates accommodating 2.0- and 2.4-mm screws Antibiotic irrigation consisting of: Normal saline 500 mL Polymyxin or bacitracin 500,000 units Cottonoids soaked in dilute epinephrine solution (1:100,000 dilution) |
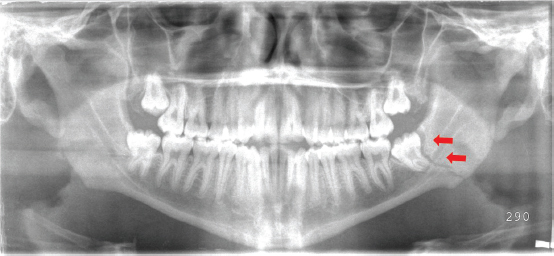
Preoperative examination should include a thorough assessment of occlusion, the dentition, and fracture mobility with bimanual manipulation. The function of the mental nerve should be assessed as well, as any fracture crossing the inferior alveolar canal can result in neurosensory deficits in the lower lip and chin. Although computed tomographic (CT) imaging is standard in facial fractures, most mandibular injuries are adequately assessed with a panoramic x-ray (Panorex) (Figure 14.1) and an anteroposterior (AP) view.
PREOPERATIVE MARKINGS
Preoperative marking depends entirely on the approach to the fracture. Simple fractures are best treated through an intraoral incision in the gingivobuccal sulcus. Complex fractures are often best treated through an external incision in the neck. This should be marked approximately two finger-breadths below the inferior mandibular border. This prevents the incision from riding up to the level of the cheek when the patient is upright.
INTRAOPERATIVE DETAILS
At the beginning of the procedure, the incision should be made and the fracture site exposed and grossly reduced. Most fractures of the mandible can be accessed through a vestibular incision.
When using an intraoral incision, great care must be taken to avoid injury to the mental nerve. In addition, an adequate cuff of mucosa must be left attached to the mandible to allow closure. When using an extraoral incision, once the level of the platysma is reached, a hemostat should be used to spread deep to it before resecting with the eletrocautery to avoid damaging the marginal branch of the facial nerve. Usually, this can be found crossing the mandibular border at the level of the facial artery and vein.
Cottonoids soaked with dilute epinephrine solution are placed in the operative site and attention is turned to the arch bars. The fracture should be reduced at this point.
Arch bars should be applied on the upper and lower dentition using 26-gauge circumdental wires from at least the first bicuspid through the second molar. Generally, the incisors are not utilized for the wire placement due to concerns regarding potential tooth extrusion.
The intermaxillary fixation should be achieved with either elastics or with wire to reestablish what appears to be the pre-injury occlusion (Figure 14.2).
Fracture fixation is a secondary goal after occlusal stabilization. Anatomic reduction of a mandibular fracture is facilitated by maxillomandibular fixation.

Related posts:
 12 Cleft palate repair: The Furlow double-opposing Z-plasty, the Von Langenbeck palatoplasty, and the V-Y pushback palatoplasty
12 Cleft palate repair: The Furlow double-opposing Z-plasty, the Von Langenbeck palatoplasty, and the V-Y pushback palatoplasty
 13 Orbital floor fracture
13 Orbital floor fracture
 15 Zygomatic and zygomaticomaxillary complex (ZMC) fractures
15 Zygomatic and zygomaticomaxillary complex (ZMC) fractures
 11 Unilateral and bilateral cleft lip repair
11 Unilateral and bilateral cleft lip repair
 1 Skin grafting and dermal substitute placement
1 Skin grafting and dermal substitute placement
 16 Non-surgical facial rejuvenation with neuromodulators and dermal fillers
16 Non-surgical facial rejuvenation with neuromodulators and dermal fillers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


