11 Unilateral and bilateral cleft lip repair
INDICATIONS
Presence of cleft lip
Desire for improved nasolabial appearance and function
Residual secondary cleft lip deformities:
Inadequate weight gain due to poor feeding
Difficulties with speech
Poor self-esteem due to appearance
Malocclusion of the teeth
INTRODUCTION
Cleft lip malformations are due to embryologic alterations in the fusion of the frontonasal and maxillary prominences of the first branchial arch. Included anatomic malformations include discontinuity and anomalous insertion of orbicularis oris and altered naso-pharyngeal development. 1 This results in poor feeding, subsequent inadequate weight gain, as well as speech difficulties. Cleft lip consists of a spectrum, including microform clefts, unilateral incomplete, unilateral complete, bilateral incomplete, and bilateral complete types. Incomplete clefts are characterized by the orbicularis discontinuity without involvement of the nasal vestibule. Complete clefts involve the nasal vestibule and alveolar ridge and may extend onto the palate. When correcting this deformity, plastic surgeons should keep in mind not only the three-dimensional flap rotations but also the “fourth dimension” of the effect of time and growth on the repair. 2 Our preferred operative techniques are based on a low complication rate and decreased visibility of scarring with selected procedures. Table 11.1 and Figure 11.1 indicate special equipment needed.
Preoperative antibiotics: cefazolin 25 mg/kg IV or clindamycin 20 mg/kg IV (optional) Double-prong hook Single-prong hook Supersharp® Micro Feather disposable ophthalmic scalpel with plastic handle #11 blade #15c blade Castroviejo surgical caliper 25-gauge hypodermic Adson-Brown forceps Methylene blue (for preoperative markings) 30-gauge needle Senn-Muller surgical retractor 4-0 Monocryl® (Ethicon, Somerville, NJ) or equivalent 5-0 Prolene® (Ethicon) or equivalent 4-0 chromic gut 4-0 Vicryl Rapide™ (Ethicon) or equivalent Lidocaine (1%) with epinephrine (1:200,000) |

ANATOMIC LANDMARKS IMPORTANT TO CLEFT LIP REPAIR (FIGURE 11.2)
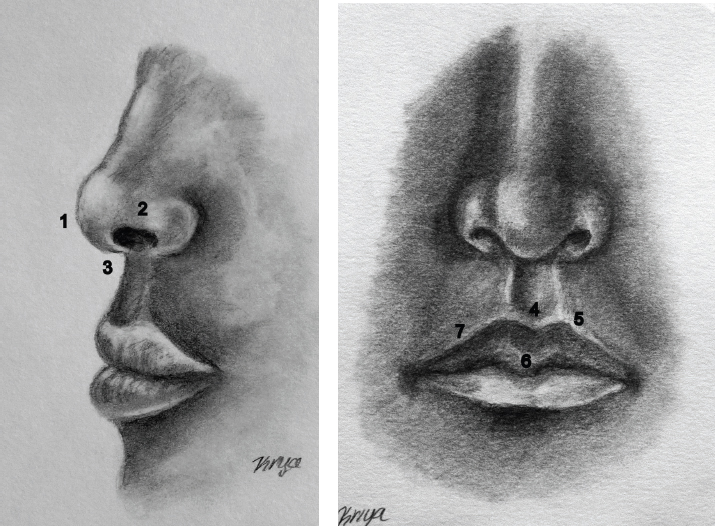
Nasal tip: The point of the nose created by the midline abutment of the greater alar cartilage apices.
Nasal ala: Formed by greater alar cartilages and fibro-fatty connective tissue; it defines the nasal vestibule.
Columella: The midline central “pillar” of the nose formed by bilateral medial crura of the nasal cartilages, nasal septal cartilage, and anterior maxillary spine.
Philtrum: The midline portion of the upper lip defined by the central depression; it is also termed the infranasal depression or philtral dimple. Borders of the philtrum are the philtral columns.
White roll: The prominent border between cornified squamous epithelium of the lip and the vermillion border.
Median tubercle of the lip: The median vermillion prominence of the upper lip.
Cupid’s bow: Describes the curved shape of the epidermal-vermillion border junction of the upper lip at the philtrum. Philtral columns adjoin the two “peaks” of the Cupid’s bow.
ASSOCIATED ANATOMIC MALFORMATIONS (FIGURES 11.3 AND 11.4)
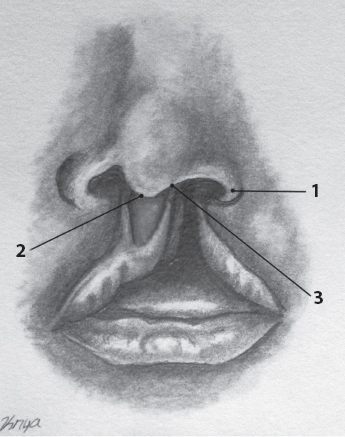
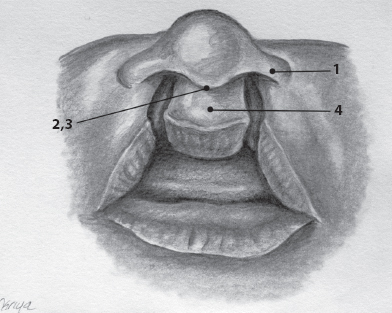
Flattened and widened ipsilateral nasal alar cartilage; is on both sides in bilateral clefts.
Rotated nasal tip in unilateral clefts; flattened nasal tip in bilateral cleft lip.
Shortened rotated columella, toward the cleft side.
Downturned ipsilateral nostril.
Prolabium: The undifferentiated nasofrontal tissue found in bilateral complete clefts used to reconstruct the philtrum.
Patient positioning
After the induction of general endotracheal anesthesia, the tube is secured in the midline. Temperature, oximetry, electrocardiogram (ECG), blood pressure, and respiration monitoring should be in place, as well as placement of active warming devices. The patient is positioned on a Philippine board with the head suspended off the end in an extended position on a gel donut or head roll. Eyes are lubricated and taped closed. We prefer to use Tegaderm™ (3M, St. Paul, MN) to keep any blood and Betadine® (Purdue Products, Stamford, CT) out of the eyes. After this, the face is prepped with Betadine paint.
UNILATERAL CLEFT LIP REPAIR
The preferred method is an adaptation of advancement-rotation unilateral cleft repair because of its re-creation of Cupid’s bow and avoidance of philtral flattening. 3 In addition, the incision lines are hidden within the nasolabial sulcus and simulated philtral ridge. Malformation can be conceptualized as medial and lateral elements. Medial elements are rearranged to re-create the philtrum and philtral ridge. Lateral elements are separated into the nasal elements and lateral flap. Nasal elements are brought medially to reshape the nasal flattening. Preoperative markings are shown in Figure 11.5.
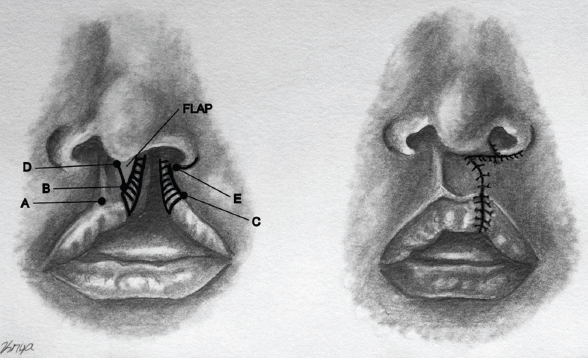
Identify the midline of the planned philtrum at the epidermal-vermillion border. Mark the non–cleft-side peak of Cupid’s bow at the base of the philtral column (point A), then an equidistant point from the midline toward the cleft side along the epidermal vermillion border (point B). A curvilinear line between points A and B creates the handle of Cupid’s bow. The total distance between points A and B should be between 3 and 4 mm; this can be tailored to the patient’s facial and ethnic proportions.
Mark the proposed peak of the Cupid’s bow on the lateral complex of the cleft side (point C). Point C will meet point B in closure. This point can be determined by locating the point on the lip where the vermillion is thickest and the white roll begins to fade. The distance from point A to the non–cleft-side commissure should be equal to the distance from point C to the cleft-side commissure.
Mark along the junction between the philtrum and columella approximately two-thirds its width on the non–cleft side (point D). Then, mark a convex curvilinear line between this point and point B. This line separates the proposed columella from the medial cutaneous flap (depicted by gray shading in Figure 11.5) from the proposed philtrum; this incision line allows rotation of the philtrum inferiorly and lengthening of the cleft side. Further rotation of the proposed philtrum can be achieved with a back cut extending from point D toward the peak of the Cupid’s bow on the non–cleft side; this back cut should run parallel to but not cross the non–cleft philtral column. Mark along the epidermal-vermillion border lateral to the medial cutaneous flap; this incision creates the lateral vermillion flap.
Mark along the lateral border of the ala and extend to the mucocutaneous junction, then extend caudally along the white roll to point C. This creates the lateral cutaneous flap and lateral vermillion flap; the apex of the lateral flap will be point E; this will meet point D on closure.
The length of point C to E should be equal to the length from point B to D.
Intraoperative details
After creation of the marks, inject lidocaine with epinephrine along the marked lines.
DISSECTION OF MEDIAL ELEMENTS
After allowing adequate time for epinephrine to take effect (7–10 minutes), incise the lines using the Supersharp ophthalmic blade. Incise the vermillion epidermal junction of the medial cutaneous flap.
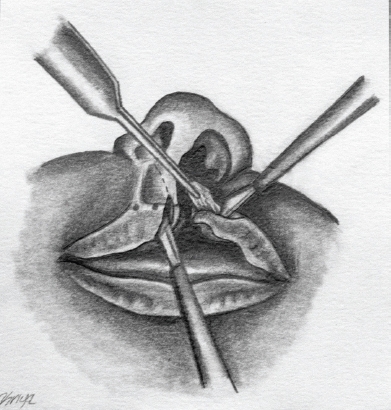
Complete the incisions with a #11 blade. Use double-prong skin hooks for retraction and elevation of the flaps. Start with the philtral rotational flap by incising between points B and D. Using skin hooks for retraction, dissect the philtral flap and medial cutaneous flap away from the orbicularis oris (Figure 11.6).
Complete the dissection of skin and vermillion flaps away from the orbicularis oris.
Incise the anomalous medial insertion of orbicularis oris on the columella.
Related posts:
 12 Cleft palate repair: The Furlow double-opposing Z-plasty, the Von Langenbeck palatoplasty, and the V-Y pushback palatoplasty
12 Cleft palate repair: The Furlow double-opposing Z-plasty, the Von Langenbeck palatoplasty, and the V-Y pushback palatoplasty
 14 Mandible fracture management
14 Mandible fracture management
 13 Orbital floor fracture
13 Orbital floor fracture
 15 Zygomatic and zygomaticomaxillary complex (ZMC) fractures
15 Zygomatic and zygomaticomaxillary complex (ZMC) fractures
 1 Skin grafting and dermal substitute placement
1 Skin grafting and dermal substitute placement
 19 Brow lift
19 Brow lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


