Summary
The ability to provide contour to the body by adding or removing adipose tissue provides the cosmetic surgeon with a power tool to meet the needs of their patients. For the face and neck, there are special considerations that need to be observed in order to ensure optimal outcomes while minimizing risks. The following chapter will help to describe the techniques to address important areas on the face, submental area, neck and other anatomic areas as well as how to manage any complications should they arise.
14 Liposuction
14.1 Background
Liposuction removes focal adipose accumulation improving localized body contour. Traditionally, liposuction, which entails vacuum-assisted transcutaneous cannula suction of subcutaneous fat using a crisscross or triangulation pattern and multiple port sites, was performed exclusively under general anesthesia or conscious sedation. The advent of liposuction under local anesthesia alone began in 1987 with Jeffrey Klein who pioneered tumescent technique with an extremely dilute solution of lidocaine and epinephrine. This allowed for reduced complications related to intraoperative blood loss and overall increased safety. Other recent developments in liposuction technology have increased its ease, speed, and versatility.
However, consumer data shows a decrease in the overall number of liposuction procedures in favor of noninvasive body sculpting modalities. These include radiofrequency, ultrasound, cryolipolysis, and laser fat reduction treatments. Patients appear to prefer procedures with lower recovery time and few side effects, even at the cost of achieving only mild-to-moderate results with a series of multiple noninvasive treatment sessions as compared to a dramatic benefit after a single liposuction procedure.
Consideration of patient preferences and needs through the preoperative and postoperative periods, along with planning the procedure at a point in time that is best for the patient, can help ensure postprocedure compliance that leads to an optimal result. Providers should be familiar with the changing technologies and patient choices pertaining to body contouring so that they can best address the common combination of localized skin laxity and excess adipose tissue. Prevention, minimization, and management of adverse events remain important. In this chapter we will focus on addressing contouring of the face and neck through liposuction while ensuring patient safety.
14.2 Preoperative Evaluation
As with any surgical procedure, preoperative evaluation is essential for reducing risk and ensuring good outcomes. A thorough history should be elicited that includes reasons for seeking treatment, patient expectations of treatment, past medical history, current medications and oral supplements, any potential factors contributing to poor wound healing (e.g., diabetes, chronic renal insufficiency, uncontrolled hypothyroidism, poor nutritional status, poor scar appearance), assessment of bleeding risk, and likelihood of compliance with postoperative instructions.
While diabetic patients using insulin pumps have recently been shown to develop paradoxical adipose hypertrophy of treated areas with noninvasive cryolipolysis, this has not been reported with liposuction. Diabetics are generally at greater risk of infection and poor wound healing.
Medications that should be avoided prior to liposuction include anticoagulants, nonsteroidal anti-inflammatories (NSAIDs), and supplements that have anticoagulant properties such as gingko, ginseng, garlic, saw palmetto, feverfew, and fish oil. Phytocoumarins can also interact with anticoagulants and other medications to increase the risk of major bleeding events. 1 , 2 Medications and supplements that can potentiate bleeding should be discontinued 2 weeks prior to liposuction. Alcohol should also be avoided.
Careful and meticulous documentation of the discussion of the risks and benefits of the procedure along with substances to avoid is an essential part of the informed consent procedure. In addition, ensuring a patient understands the likely degree of postprocedure contour improvement is critical for patient satisfaction.
Absolute contraindications to liposuction include severe obesity, a patient seeking the procedure as a weightloss solution, body dysmorphic disorder, and scarring or altered anatomy from prior surgery in the area. Consideration of earlier keloidal scarring, bleeding episodes, allergic reactions to lidocaine, incidences of poor wound healing, and unstable psychiatric condition may lead to a decision not to proceed, thereby helping prevent avoidable adverse events and patient dissatisfaction.
Appropriate patient selection greatly increases the likelihood of subsequent patient satisfaction. Patients who do not have reasonable expectations of the likely cosmetic benefits of the procedure, demand guarantees of success, or see the procedure as a way to solve a life challenge are not ideal candidates. All patients should be advised that a “touch-up” may be needed. Preoperative discussion should identify those who, regardless of the result, will not be satisfied or will be unwilling to engage in additional adjunctive treatment to achieve the desired aesthetic goal. In some cases, noninvasive modalities for fat reduction may be appropriate alternative treatment avenues.
Written preoperative and postoperative instructions are typically provided to the patient along with verbal communication of the most common and important adverse events. It is helpful to provide recommendations on nutrition and exercise to help with maintenance of results. Consultation with experts in these areas may be sought when appropriate. Lifestyle changes may need to be implemented prior to the procedure. The best results are seen in those who are at or slightly above their stable body weight. Extreme dieting prior to liposuction is highly inadvisable, as patients are likely to gain this weight back postprocedure, even if not at the anatomic site that underwent treatment. Ultimately, provision of emotional support of the patient from the time of preoperative consultation until after the postprocedure recovery leads to greater patient satisfaction.
14.2.1 Physical Examination and Laboratory Evaluation
For facial and neck liposuction, the surgeon identifies the high and low contours along with free margins and aesthetic subunits. The main areas of concern are the pretragal sulcus, nasolabial fold, malar fat pad, neck, and submental fat (Fig. 14.1). It can be helpful to use a skin marker to identify, fully visualize, and then confirm with the patient, the primary areas of concern. Scars or traumatic wounds that may restrict postoperative skin contraction should be identified and shown to the patient. For submental fullness, assessment of skin laxity, platysmal laxity, anterior digastric hypertrophy, and adipose collection at the site allows the generation of a complete plan to treat these diverse elements. The masseter muscle and the overlying malar fat pad largely account for the cheek and jaw contour. The pretragal sulcus and nasolabial folds are less impacted by the underlying anatomy. Skin laxity can be assessed by the “snap test” where gently pulling on and then releasing the skin at the neck or area of interest shows the ability of the skin to easily return to its original position. A longer time to return to back to its original position (i.e., positive snap test) predicts an increased likelihood of persistent laxity after the liposuction procedure.

The surgeon is aware of the angles (e.g., cervicomental angle) and depressions that are considered youthful and natural for the patient’s ethnic background, gender, and social group. For example, Western cultures prefer oval face shapes in women and more squared jawlines in men, while Asian cultures prefer an oval face shape with V-tapered jawline down to the point of the chin. 4 Correction outside of these norms may lead to a suboptimal result, and a dissatisfied patient. 5
Baseline photographs are taken in profile without neck extension, oblique at 45 degrees with the nasal tip on the cheek, and portrait view to show all the relevant contours and depressions for later comparison. Software is available to simulate typical results, which can aid the preoperative discussion. Recognition of the need for platysmaplasty, partial resection of the anterior belly of the digastric muscle, or surgical neck lifting in conjunction with liposuction may also contribute to selection of an optimal treatment approach. Preoperative ultrasound of the neck can assist in distinguishing skin or fat abnormalities from problems arising from muscle dysfunction. 3 While there are no data to support anterior digastric muscle neuromodulator injections to reduce submental fullness, this may still be considered by some. Cases have been reported of such injections used to address hypertrophy from traumatic overbite. Caution should be exercised if attempting to surgically reduce anterior digastric bulk as this muscle is involved in speaking and chewing. Any attempt to manage muscle mass, as well as scar modification by laser or surgery, may need to be completed prior to correction of fat deposits. For cheeks or malar fat pads, masseter hypertrophy is typically managed with neuromodulators prior to evaluating a patient as a candidate for liposuction.
Further aspects of preoperative planning include obtaining vital signs, assessing the volume of tissue to be removed, measuring weight and BMI, testing local neuromuscular function, and checking the level of vascular perfusion. Documenting a baseline neuromuscular evaluation allows for comparison in the postoperative period if there is a question of nerve injury. Any indications of compromised, altered, or atypical vascular anatomy in the area of the procedure are documented. While surgical technique is planned in a manner to avoid vascular injury, atypical anatomy can increase such risk during the procedure. Basic laboratory blood testing, including CBC, electrolytes, creatinine, INR, PTT, hepatitis B and C, β-hCG, and HIV, is suggested. This is especially true if larger volume liposuction is planned. An electrocardiogram and other tests of the cardiovascular or pulmonary systems may be relevant in the context of particular patient comorbidities.
14.2.2 Anesthetic Planning
Selecting an anesthetic plan is a key preparatory step. Tumescent anesthesia without general anesthesia is believed to be the safest method to perform liposuction as it avoids risks and complications associated with general anesthesia. Patients are also able to assist the surgeon by indicating any feelings of pain or discomfort when the surgical plane is too superficial or there is a pending thermal injury from energy-based devices. If general anesthesia is chosen due to the need for concurrent adjunctive surgical procedures, the patient should be counseled regarding the increased risks of cardiovascular issues, venous thrombosis and vascular complications, and skin injury and delayed healing. For awake analgesia, tumescent liposuction with 55 mg/kg of patient body weight is known to be safe. This dose is recommended by the American Society for Dermatologic Surgery based on existing safety data in the literature. 6 Klein and Jeske have recommended 45 mg/kg for liposuction to increase the margin of safety. 7 However, there is no evidence that levels even greater than 55 mg/kg are unsafe, and the reluctance to use these is based more on the absence of confirmatory safety data than any reports of adverse events with higher doses. Each IV bag of tumescent solution typically contains 1 g lidocaine with 1 mg epinephrine in 100 mL, plus 10 mEq of 8.4% sodium bicarbonate in 10 mL, both added to 1,000 mL of 0.9% saline. In the context of diabetes or hypoalbuminemia, treatment with macrolides (given associated CYP3A4 or 1A2 inhibition), fluoroquinolones, or selective serotonin reuptake inhibitors, and use of lidocaine without epinephrine or general anesthesia (see Table 14.1), a larger margin of safety may be preferable. In these cases, it has been suggested that the maximum tumescent lidocaine dose be 45 mg/kg. 7 A simplified method to calculate the maximum safe volume is: [dose of lidocaine × weight (kg)/10] × [1/concentration of lidocaine]. 8 For a patient of average weight (approximately 70 kg), approximately 4 L of 0.1% lidocaine tumescent fluid is considered safe. Delivery of the solution is typically through a power-assisted infusion cannula, or 60-mL syringe for smaller areas. The syringe-based method is often useful for the face and neck.
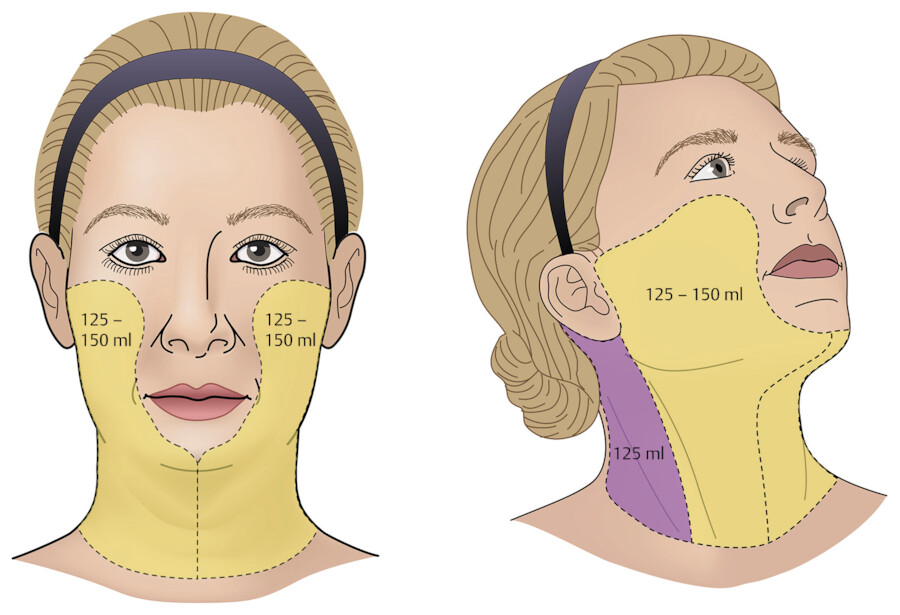
Though volumes may vary, the cheek and neck often require 125 to 150 mL of tumescent fluid for each side. The postauricular areas and posterior neck may take 125 mL per side. Therefore, for a typical bilateral facial procedure approximately 600 mL of tumescent lidocaine may be appropriate (Fig. 14.2). Smaller volumes infused with a syringe may be best for the pretragal area and nasolabial folds if one of these is the only area of concern.
Some patients may require preoperative oral analgesia, light sedation, anxiolytics, and antiemetics to tolerate the procedure. The decision to administer additional medications in the setting of tumescent liposuction should be individualized. Many patients who are nervous about the procedure can be guided through liposuction successfully with reassurance and distraction techniques.
14.2.3 Selecting the Right Tools to Optimize Aesthetic Results
Body contouring has undergone a paradigm shift in recent decades, with a renewed understanding of the distinction between fat reduction on the one hand, and tightening of adjacent skin and muscle, on the other. The evolution of technology to permit the surgeon to address all the relevant soft tissue layers has allowed for better overall outcomes. In many cases, combining various modalities may be best for achieving optimal results.
Traditional cannula and vacuum-assisted suction remains the mainstay of body contouring. Suction cannulas are hollow metal tubes with blunt patient-facing ends and holes near distal tip. Cannulas are manufactured in various bores as well as in different lengths, and also differ in the number, shape, configuration, and size of their holes. Specialty cannulas may have a circumferential array of holes for fat harvesting, or forked blades for lysis of fascial or subcutaneous adhesions. Fat reduction by cannula typically occurs via manual mechanical tunneling or power-assisted oscillation. Mechanical removal is by the physical disruption of the adipose structure into lobules, the additional benefit of hydrosection if tumescent anesthesia is used. The skill of the surgeon guides maintenance of an adequate surgical plane and sufficient force to remove the fat. To avoid oversuctioning of a small area, the suction cannula is moved back and forth in long strokes comprising most of its length, and in a fanning motion laterally. The vibratory action of an oscillating cannula facilitates passage through subcutaneous tissue, thereby sparing some physical effort for the surgeon. Vibration also speeds adequate treatment of fibrous regions or areas of prior surgery, provides vibratory sensory stimuli to distract the patient and increase comfort, and may reduce the risk of shearing adjacent tissue.
Energy-assisted liposuction with radiofrequency, ultrasound, 1,064-nm laser, or 1,470-nm laser has been reported to increase the pace of removal, purportedly by liquefaction or destruction of the fat prior to suctioning. Further, use of energy devices may contribute to skin tissue shrinkage and sculpting of the cosmetic subunits in “high-definition” procedures that even etch the underlying muscle. Some degree of targeted skin tightening may thus be achieved in a single procedure. Energy device used in combination with liposuction delivers either heat or shock-wave-based disruption of the fat lobules. For tightening of the overlying skin, the local skin temperature needs to reach approximately 46 °C. Nonthermal ultrasound may thus not achieve as much skin tightening as radiofrequency, infrared laser, or thermal ultrasound. The disadvantage of delivering heat during liposuction is an increased risk of subcutaneous thermal injury to the skin and dermal plexus vessels. Thermocoupled devices that provide real-time temperature feedback to the operator are available to reduce the risk of injury. If fat transfer of the lipoaspirate is being considered, then traditional or nonthermal ultrasound-assisted liposuction may be considered as they may preserve a higher fraction of viable autologous fat and stem cells for grafting. In using energy devices with traditional liposuction, the operator needs to be familiar with their benefits and risks, and able to prevent thermal injury to the skin and vasculature.
Inappropriately superficial liposuction can increase the risk of skin injury. So-called “high-definition” techniques offer accentuation of the edges of aesthetic landmarks and muscle boundaries by using cannulas to etch the skin or muscle while attempting to preserve the subdermal plexus. Additional familiarity with this approach is advisable before employing it in a live patient.
The overall benefits of body contouring associated with liposuction can be increased in magnitude with the adjunctive use of noninvasive or minimally invasive modalities such as energy-device actuated skin tightening. For those patients who are poor surgical candidates or desire a shorter recovery, noninvasive or minimally invasive modalities may be used as solitary treatments, albeit with the expectation of less noticeable results or the need for an increased number of treatments. Nonsurgical reduction of adipose tissue using physical modalities (i.e., heat, cold, shock-waves) can be accomplished using cryolipolysis, external and internal radiofrequency heating, thermal and nonthermal (shock-wave) ultrasonographic adipolysis, and infrared (commonly Nd:YAG 1,064 nm) laser lipolysis. Indirect comparison of clinical studies shows a comparable reduction in adipose tissue volume of approximately 20 to 25% after a series of treatments with each of these methods. The best results are in those who have focal fat deposits and a BMI < 30.
Interestingly, despite the lack of heat delivery, cryolipolysis appears to be able to achieve an adjunctive reduction in skin laxity. It has been postulated that dermal fibroblasts may initiate collagen deposition in the skin due to the stretching and suction of the cryolipolysis device or cold stimulation. Heat-based laser, radiofrequency, and ultrasound devices use long wavelength energy to induce an adequate temperature for fat destruction while avoiding inducing thermal injury of the skin. External ultrasound or radiofrequency devices that target the deep dermis and fascia specifically are sometimes used with heat-based liposuction devices. In addition to serving as primary treatment modalities, noninvasive and minimally invasive fat reduction methods may also be useful for fine-tuning, adjusting, or touching up the results of a liposuction procedure.
Additional adjunctive techniques can improve body contour before or after liposuction. Specifically, postoperative electromagnetic stimulation (EMS) of the underlying muscle has been reported to facilitate skin tightening. EMS has shown effectiveness in reducing abdominal ptosis and narrowing the diastasis recti. Clinical studies have used treatment protocols of four treatments divided over 2 weeks, with a twice a year maintenance schedule for the abdomen. Early data suggests augmentation of liposuction results for the abdomen if EMS treatment is started within 48 hours after the procedure. Data on the face are more preliminary.
Laxity of the face and neck can be treated by other modalities as well. Definition of the jawline may be sharpened with neuromodulator application along the lower face. Since platysmal laxity or digastric hypertrophy may contribute to submental fullness and suboptimal neck contours, neck rhytides may be reduced with neuromodulator application when platysmal bands are present. The platysma may be surgically addressed by either platysmaplasty (e.g., corset platysmaplasty) or a minimallyinvasive percutaneous approach. 7 , 9 There are no controlled studies regarding these procedures.
14.3 Procedure
14.3.1 Cannulas
Cannulas differ in length from 3 to 14 inches and vary in bore from 10- to 18-gauge. The bore, cannula hole characteristics, and tip architecture correlate to the level of aggressiveness the cannula can provide. Medium-to-low aggressive cannulas (Table 14.2) are most useful for finely sculpting an area with small fat deposits to ensure controlled, precise removal. Aggressive cannula designs like the Keel Cobra are generally used for debulking on nonfacial body sites when a large accumulation of fat is present. A helpful rule is that aggressive cannulas tend to be higher gauge, more tapered at the point, and possess larger holes near the tip. Ensuring that the cannula holes remain on the ventral side during suctioning can help to reduce the chance of skin dimpling. On the face and neck, short, fine bore cannulas, such as the 3-inch 18-gauge, are commonly used. These are sufficient because of the small volume of fat needing to be removed, and are helpful for minimizing trauma to the abundant important superficial neurovascular structures.
14.3.2 General Principles of Surgical Technique
Suction techniques for each area of the head and neck are similar; however, there are subtle site-specific differences in the selection of appropriate cannula (Table 14.3). Treating multiple contiguous locations during the procedure can prevent sharp cutoffs or lines of demarcation, and blend the face or neck shape. Similarly, triangulation, or suctioning the site from two or three distinct entry points, helps minimize the risk of contour deformities and contributes to an overall even contour.
Aggressiveness | Type | Size |
High | Capistrano Keel Cobra Mercedes Pinto Toledo | 10 or 12 G 3 or 3.7 mm 10 or 12 G 10 or 12 G 10 or 12 G |
Medium | Capistrano Klein Accelerator/Triport Dual Port Fournier Keel Cobra Texas | 14 G 12 G 3 mm 2.5 mm 2.5 mm 2.5 mm 2.5 mm |
Low | Capistrano Klein Spatula | 16 G 14–18 G 2–3 mm |
After photographs are taken, treatment areas are marked and the patient is sterilely prepped and draped. For the neck and submental areas, a supine position with neck hyperextension is preferred. Some surgeons prefer elevation of the head to 45 degrees to facilitate a natural line of cannular insertion from the mentum down the neck. Port holes are made by incision or a punch biopsy tool (1-, 1.5-, or 2-mm punch) in areas that are easily hidden or along relaxed skin tension lines. For the neck, these sites are typically an inch below the pinna and slightly recessed below the point of the chin beyond the terminal lip of the jaw. Tumescent anesthesia is administered by blunt needle or spinal catheter attached to a 30- or 60-mL syringe. While warmed fluid is used to minimize the risk of hypothermia in larger cases, this is not typically necessary on the head and neck. Warming may also encourage bleeding due to vasodilation. Passive warming of the patient with blankets, or active warming with a forced warm air blanket, may be preferred. The rate of infusion of tumescent fluid is typically 100 mL/min with a 30- to 45-min delay after infusion and before suction for full anesthesia to set in. Blanching of the overlying skin will occur when anesthesia has taken full effect. The subdermal area, mid-fat, and deep fat should all be infused. Laterally, an area about 1 inch beyond the area to be treated should be infused, and should be blanched prior to the start of suction.
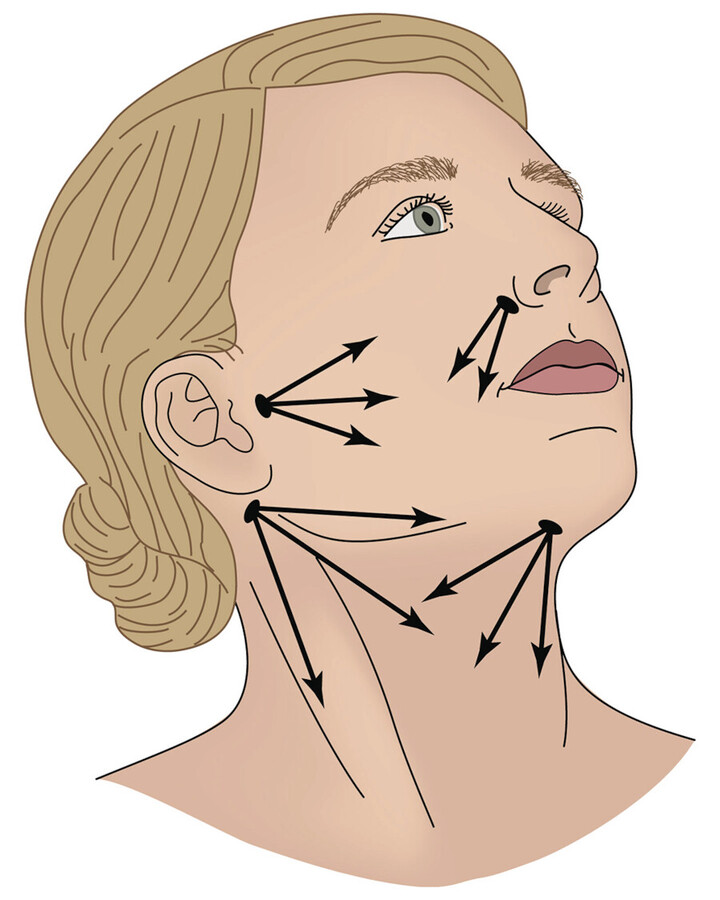
The suction cannula is inserted nearly vertically at first, and then quickly leveled to an angle of 20 to 30 degrees to avoid injury to deep structures. After the cannula is safely inserted into entry port, it is advanced radially to create tunnels, like the spokes of a wheel (Fig. 14.3) into the areas that were premarked for treatment. Pinching of the skin with the nonoperative hand to tent the subcutaneous tissue allows for maintenance of a consistent depth. The surgeon should control the cannula with their dominant hand while their guide hand folds the skin over the cannula. Pinching of the skin and guiding the cannula to pierce through the pinched tissue bulk decreases the depth of aspiration; on the other hand, pinching with the palm and then guiding the cannula below the pinched tissue increases the depth of treatment. Such maneuvers guide the depth of the cannula tip to remove fat from the different depths of adipose layer. Changing between grips is more important for areas on the trunk and extremities, but can be useful also for areas of increased fat density on the head and neck. During the tunneling process at delicate sites, suction is minimal and any energy-based assistance is kept off. Once initial tunneling is completed, the more assertive suction removal can start. As a general rule, overcorrection should be avoided as this can create contour deformities and a skeletonized look or overlying skin rippling and dimpling. When there is doubt regarding the prudence of further fat removal, it is recommended that the operator pauses and assesses the progress of the procedure. More fat can always be removed later. “Feathering,” or more conservative fat removal at the margins of a cosmetic unit or subunit, helps blend the overall results without leaving demarcation lines between cosmetic units.
During the procedure, the surgeon should be mindful of the character of the aspirate being removed. A pale, straw-colored to yellow aspirate is ideal. Some serosanguinous fluid mixed within the aspirate is acceptable. Frank blood should lead to a reassessment of cannula position and active exploration to ensure no major vessels have been injured. When vigorous suction with repeated readjustment of the angle and direction of the cannula yields little to no aspiration of additional fat, treatment at that site is likely completed.
14.3.3 Malar Fat Pad and Cheek Contouring
The typical patient may complain of increased cheek fullness that causes them to appear puffy or overweight. This manifestation of cheek enlargement can occur for a variety of reasons, including normal interpersonal variation, but it may also be related to weight elevation, metabolic disease, or medications. Before liposuction is considered, it is appropriate to consider any exacerbating factors that can be modified without surgery through counseling, behavioral change, or medication management. Masseter hypertrophy, which may reduce the benefit of a liposuction procedure, may be treated with neuromodulator injections.
Entry points for facial liposuction are typically preauricular and perinasal. Alternatively, direct needle aspiration of subcutaneous fat can be performed. Keeping entry points away from the midcheek most effectively conceals any associated scar. The surgeon should be careful not to overcorrect the cheek, thereby engendering a sunken look and risking aging the face by removing natural structural support. A “touch-up” procedure can always be performed months later, once a steady state devoid of postprocedure edema is observable, should more fat removal be required. Typical cannula types for the head and neck are of low-to-medium aggressiveness, commonly Capistrano or Klein (i.e., spatula) tips of 1 to 2 mm diameter. Smaller cannulas are used for feathering toward the edges of the fat pad and sculpting of depressed areas like the pretragal sulcus that define the cheek. Combination treatment with rhytidectomy may be selected when significant skin laxity, sagging, and jowling is present. Concomitant rhytidectomy provides the advantage of direct visualization of the lateral aspects of the malar pad.
14.3.4 Treatment of the Nasolabial Fold and Pretragal Sulcus
The nasolabial fold and pretragal sulcus can be treated with a 1- to 2-mm cannula to create natural folds that are blunted by fat accumulation. Gradual fat removal is desired, with frequent checking of the intraoperative result to prevent overcorrection. Treatment of these areas is often combined with treatment of other nearby areas, such as the jowl of malar fat pad. Sculpting of the elevated portion of nasolabial folds to soften and smoothen excessive deepening may be accompanied by lysis of any adhesions to mimetic muscles by blunt dissection with the cannula to provide a gently undulating contour. 8 , 10 Correction of lateral volume loss with hyaluronic acid injections or rhytidectomy should be considered when appropriate. Care should be taken prior to suctioning adjacent to a deepened nasolabial fold to ensure that it does not make it even deeper.
14.3.5 Treatment of the Jowl
A preoperative evaluation can determine whether the jowl is a result of excess fat deposition or mid- and lateral face age-related volume loss. In general, volume loss should be corrected by soft tissue augmentation (i.e., not liposuction) at the most superior aspect first, with subsequent lesser treatment to the inferior areas. This helps to elevate mid- and lower-face structures while accentuating the “V-shape” of the face, which is an indicator of youth. The jawline can be redefined by adding hyaluronic acid filler deeply 1.5 cm anterior to the posterior border of the mandible while retracting laterally during injection. Thereafter, use of additional filler for definition along the mandible and correction of any other depressions can be considered. Some injectors use a long 25-gauge cannula for filler injections along the posterior mandibular border but the choice of bore and length of the cannula, and the decision of whether to use a cannula or a needle, varies among experts.
If, in fact, excess adiposity is present in the lateral jowl fat pads, but this excess is modest in volume, noninvasive modalities like chemical adipocytolysis with deoxycholic acid or cryolipolysis with tips specially designed for the neck may be considered instead of liposuction. There are no comparative studies of the effectiveness of liposuction versus chemical adipocytolysis or cryolipolysis for lateral jowls. 11 , 12 Rhytidectomy may be added as an adjunctive procedure for those with significant skin laxity.
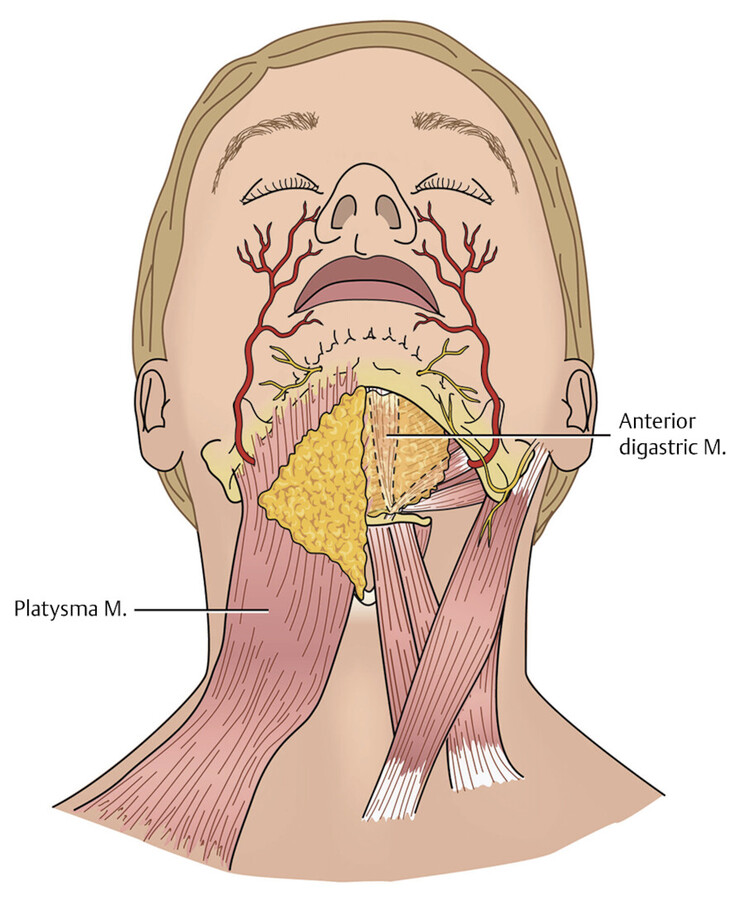
If liposuction is the preferred procedure, being mindful of the underlying anatomy will mitigate the risk of injury to the marginal mandibular nerve and facial artery along the mandibular border (Fig. 14.4). The facial artery lies approximately 3 cm anterior to the masseteric tuberosity. The marginal mandibular nerve course is complex and can vary between right and left as well as between patients. Anatomic studies vary in terms of its most inferior location—2 cm below and 0.2 cm above the mandibular border. The most common point of its crossing of the mandibular border is 2.8 cm anterior to the border of the masseter. 13 , 14 , 15 During liposuction, care should be taken to avoid cannula motions that course perpendicular to the jawline at the point where the nerve is expected to cross. If this is not done, the nerve can be snagged by the cannula, and a nerve palsy resulting in unilateral paralysis can persist for weeks to months. After avoiding important neurovascular structures, feathering and careful extraction of the adipose tissue underneath the mandibular border along with focal removal of the descended lateral jowl fat pads will provide the most aesthetic result (Fig. 14.5b). Unlike some other sites discussed in this chapter, the jowls are amenable to superficial liposuction with a high degree of safety. 16
14.3.6 Submental Liposuction
Submental liposuction begins with the creation of an entry point by punch biopsy tool or scalpel incision 1 mm posterior to the submental crease. The anatomic location of incision placement in this area is critical to prevent exaggeration of the submental crease after scar contracture during the healing process. Some surgeons support using a larger 2- to 3-mm cannula while others use a 1- to 2-mm cannula due to the benefit of the smaller entry site in the contest of the limited fat to be removed. The advantage of an incision is that a platysmaplasty or, in rare cases, the removal of the postplatysmal fat pads can be achieved if the incision is extended. Notably, platysmaplasty may cause elevation of the deep fat pad and make its removal unnecessary. Regardless of the method used to make it, the entry site should be slightly larger than the size of the cannula to reduce trauma to the skin edges.
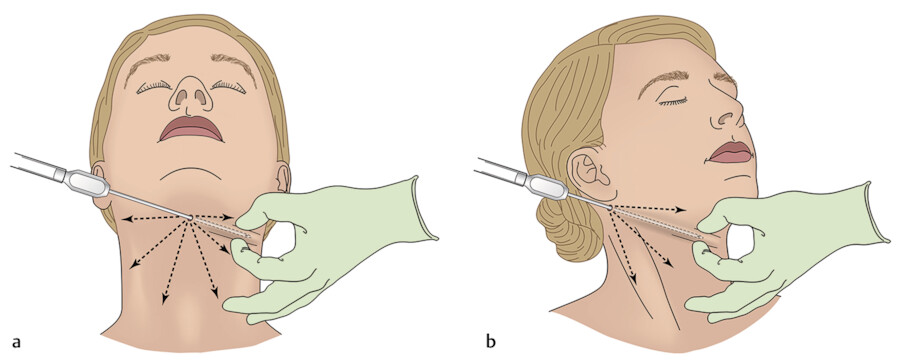
Subcutaneous cannula tunneling without suction is typically commenced to include the boundaries of the chin, anterior border of the sternocleidomastoid, and the thyroid notch. An alternative to this is blunt dissection with Metzenbaum scissors. Once the tissue has been loosened, cannula suction is initiated. Throughout the procedure, the surgeon should pause to palpate the target areas to ensure progress toward a smooth, even contour. Bulges and irregularities indicate uneven liposuction and dimpling indicates oversuctioning at a point or septal attachments that should be lysed. As the submentum lies underneath the main entry site, care should be taken to prevent overtreatment from multiple passes to treat distal sites. An excessive submental depression may simulate a “cobra” deformity, in which the oversuctioned tunnels created permit superficial tissue to contract into the new dead space. One way to avoid oversuctioning at the submentum is to turn off suction when removing and reinserting the cannula; alternatively, care can be taken to redirect the suction cannula during fanning without pulling back all the way. To assist with definition of the mandibular border, a 2-mm cannula is often used. This is rotated parallel to the mandibular border and conservative liposuction is performed. Because the marginal mandibular nerve branch and facial artery can run superficially in some patients or have atypical courses, particular caution should be exercised. The target is the fat immediately under the jawline and not over the mandibular border (Fig. 14.5a). Aspirating fat over the mandibular border reduces jaw definition. Feathering with an additional pre- or postauricular entry site helps a smoother, defined contour and also reduces the risk of a “cobra” deformity. This also aids in creating secondary fibrosis along the neckline that helps the skin contract into a tighter position, hugging the underlying muscle.
Enhancements to submental liposuction include chin enhancement or reduction, and rhytidectomy. Rhytidectomy may be needed in combination with liposuction for some patients with advanced skin laxity or extensive photodamage. Noninvasive lipolysis (e.g., cryolipolysis) can correct small residual fat deposits if they persist after the procedure. A helpful rule to measure microgenia is to hold a cotton swab vertically and perpendicular to the lower vermillion border. This demonstrates the amount of chin projection that could be corrected as the point of the chin should ideally touch the cotton swab. It is important to consider prognathia, retrognathia, and micrognathia prior to determining how much chin projection to correct. Hyaluronic acid injection or surgical revision can be performed based on the clinical situation.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


