12 Implant Technology
Summary
The original design for a breast implant was inspired by the observation that the saline in a half-filled IV bag assumed a breast-like shape. From here, the first silicone gel breast implant was created. Since breast implant’s original description, many new technologies have been developed. Three key design variables describe nearly every one of these devices and include mandril shape, shell and surface characteristics, and filling material. Understanding how these three variables mix and match allows the surgeon to better understand how these implants interact with the patient’s soft tissue to produce the desired breast size and shape. This chapter provides an overview of implant design, manufacturing and new technologies on the horizon.
Key Teaching Points
Three design variables dictate an implant’s final design.
These three variables are mandril shape, shell and surface characteristics, and filling material.
Three common methods exist for applying a textured surface to an implant surface.
Implants are available round and anatomically shaped.
New technologies are emerging in implant manufacturing.
The original design for a breast implant was inspired by the observation that the saline in a half-filled IV bag assumed a breast-like shape. From here, the first silicone gel breast implant was created, used, and subsequently reported by Cronin and Gerow in 1963. Ever since this original description, attempts to engineer a better implant to improve the performance of these devices have been made. As a result, a wide variety of different types of devices are currently available for use in aesthetic as well as reconstructive surgery of the breast. Despite the seeming complexity associated with these many different types of devices, there are only three design variables that describe nearly every one of these devices and these include mandril shape, shell and surface characteristics, and filling material. Understanding how these three variables mix and match allows the surgeon to better understand how these implants interact with the patient’s soft tissue to produce the desired breast size and shape.
12.1 Construction
12.1.1 Mandril Shape
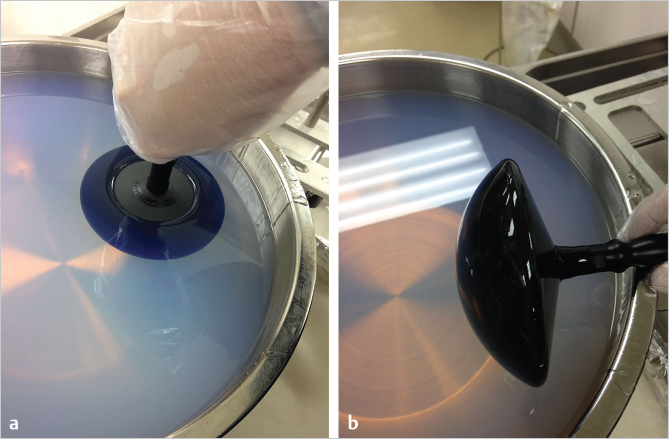
To understand how the shape of an implant can affect the subsequent shape of the breast, it is helpful to understand how an implant is made. A solid form, or mandril, is attached to a dipping rod to determine the three-dimensional outer shell of the implant. The surface of the mandril is coated with silicone by either dipping the mandril into a vat of liquid silicone or spraying a fine mist of liquid silicone onto the mandril (▶Fig. 12.1). The silicone is cured either at room temperature or with heat using a process called vulcanization that creates a solid shell. The result of this process is a breast implant shell whose shape is determined by the shape of the mandril. Repeated spray applications or dips of silicone result in a thin layer of silicone coating the mandril, thereby creating a shell of sufficient uniformity and thickness to serve as an outer form for the breast implant. Halfway through this spraying or dipping process, a phenylated silicone elastomer is substituted for the usual silicone compound. Phenylated silicone is resistant to the diffusion of silicone oil through the shell, and in this fashion creates what has been called a “low-bleed” generation of implants. This design feature eliminates the “gel bleed” phenomena, that was so common with earlier generations of implants, from occurring.
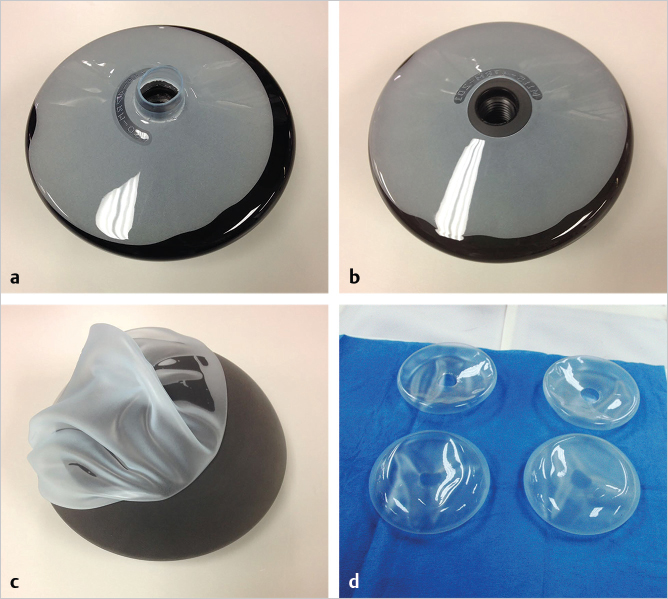
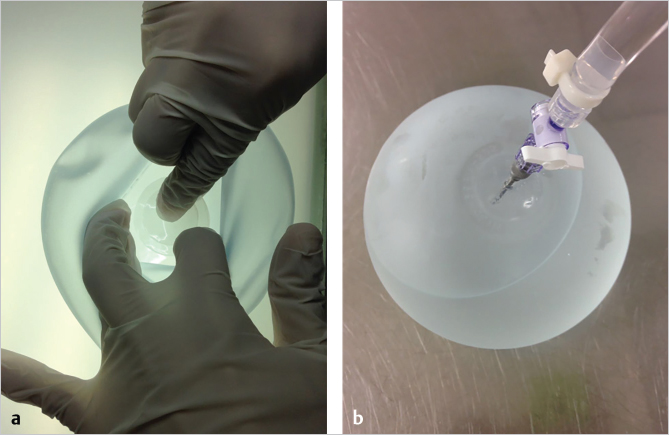
Once the shell has dried completely, the dipping rod is unscrewed from the mandril and a circular cut is made around the dipping rod attachment site. Using this as an entry point, the elastic shell is pulled off by stretching it around the edges of the mandril (▶Fig. 12.2). Next, the defect in the shell is patched with a separate piece of silicone sheeting to finish the process and prepare the implant envelope for subsequent filling with silicone gel (▶Fig. 12.3).
12.1.2 Texture
Pearl
Silicone surface textures were developed in an attempt to mimic the positive effect polyurethane foam–coated devices had on capsular contracture. The aggressiveness of these textures can be categorized as macrotextured, microtextured, and nanotextured.
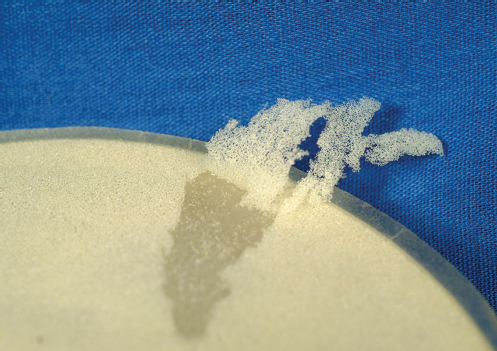
It is during the construction of the implant shell that various types of surface textures are added to the outer surface. The original silicone gel implants were constructed with a smooth surface. However, in the early 1970s, it was discovered that coating an implant with a layer of polyurethane foam resulted in an apparent reduction in the rate of capsular contracture. This was a result in part of a low-grade inflammatory giant cell response to the polyurethane, creating an ultrathin, pliable, and highly convoluted capsule. Depicted in ▶Fig. 12.4 is the polyurethane foam being pulled off a round gel implant. The thickness of the foam as well as the porous nature of the material can be seen. Unfortunately, after many years, the same low-grade inflammatory process that is presumed to prevent capsular contracture also results in a slow degradation of the polyurethane foam. Eventually, after a period of 8 to 10 years, all that is left is the underlying smooth-walled core gel implant which is associated with a slow but steady increase in capsular contracture rates.
In an attempt to mimic the effect of the polyurethane foam, texturing of the surface of silicone gel implants was developed. These textures vary in significant ways, both in roughness and method of manufacture. These textures can be subdivided into three general categories: macrotexture, microtexture, and nanotexture.
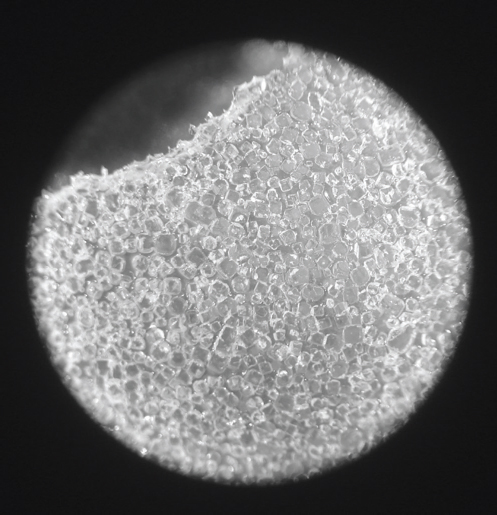
Macrotexture
Perhaps the most commonly applied strategy for creating a roughened texture on the surface of a breast implant shell is to impregnate small granules of salt or sugar into the outer surface of the shell while the silicone is still tacky and then allowing the outer implant shell to harden. When the salt or sugar crystals are subsequently washed away, an open pore lattice network is left behind that creates an aggressive macrotexture on the surface of the implant. In one version of this texturing strategy, an additional last layer of silicone elastomer is added on top of the granular coating and allowed to dry. As a last step, this outer layer is abraded away to further increase the roughness of the texture. The stereoscopic view in ▶Fig. 12.5 demonstrates such a macrotextured surface with its variably sized square-shaped pores left after dissolution of the salt granules from the surface. These macrotextures have been found to interact favorably with the capsule that develops by causing the collagen fibrils of the capsule to become intertwined with the texture of the shell. Such ingrowth occurs much more commonly with tissue expanders than with implants, because the outward force of the inflated expander tends to drive the texture into the capsule. By interlocking the capsule with the textured surface, two events occur. First, the device becomes immobile, a feature that is particularly useful when using anatomically shaped devices that must maintain the proper orientation. Second, many surgeons believe that the textured surface offers a reduced rate of capsular contracture similar to that seen with polyurethane foam. This latter finding is somewhat controversial, because several studies have failed to note a reduction in the rate of capsular contracture associated with the use of textured implants. While there may be advantages associated with such aggressively textured devices, recent studies have suggested that macrotextured implants are actually more prone to support chronic bacterial colonization in the form of a biofilm. Such biofilm formation has been implicated in the development of capsular contracture. The long-term effects of small silicone particulates that can flake away from the macrotextured device remain incompletely investigated.
Related posts:
 16 Subfascial Inframammary Breast Augmentation
16 Subfascial Inframammary Breast Augmentation
 19 Managing Asymmetry and Congenital Anomalies
19 Managing Asymmetry and Congenital Anomalies
 14 Augmentation Mammaplasty with Cohesive Gel Implants
14 Augmentation Mammaplasty with Cohesive Gel Implants
 15 Subpectoral Breast Augmentation (Inframammary Approach)
15 Subpectoral Breast Augmentation (Inframammary Approach)
 17 Transaxillary Approach to Endoscopic Breast Augmentation
17 Transaxillary Approach to Endoscopic Breast Augmentation
 11 Preoperative Evaluation of the Breast Augmentation Patient
11 Preoperative Evaluation of the Breast Augmentation Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


