Abstract
Pressure ulcers are a major concern in patient care. Left untreated, pressure ulcers can turn into pressure wounds that not only prolong healing, but additionally threaten the health and well being of the patient. Because of this, it is imperative that ulcers be promptly and properly treated. The authors take the reader through presurgical preparation and the operative interventions of debridement and reconstruction (often, flap reconstruction), to the postoperative care treatments that promote a good outcome.
11 Pressure Ulcers
11.1 Goals and Objectives
Understand the risk factors for pressure ulcers and be able to describe how they contribute to the formation of pressure wounds.
Appreciate the multimodality approach for treatment and prevention of pressure ulcers.
Be able to assess patients and optimize ancillary treatments prior to surgical intervention.
Know surgical treatment options in the setting of sacral, ischial, and trochanteric pressure ulcers.
Be able to counsel patients on postoperative treatment goals and outcomes of intervention.


11.2 Patient Presentation
A growing number of patients are presenting with pressure ulcers. Studies from Europe calculate the incidence in hospitalized patients to be 3% to more than 30%. 1 The cost of pressure ulcer treatment is estimated to be 11 billion dollars per year in the United States and utilizes 4% of the National Health Service’s budget in the United Kingdom annually (1.4–2.1 billion U.S. dollars). 2
Pressure ulcers occur in patients with impaired mobility in association with multiple risk factors. A lack of pressure relief techniques and devices places areas over bony prominences at risk (Fig. 11‑1, Fig. 11‑2, Fig. 11‑3, Fig. 11‑4) 2 : A lack of pressure relief techniques and devices place the heels at risk in bedridden and supine patients (Fig. 11‑3; Fig. 11‑4).

More worrisome is the resulting cone-shaped distribution of injury, with deeper tissues closest to the bone suffering the greatest damage. In these wounds, small-appearing superficial ulcers can have more severe injuries deep to the surface with an area of soft-tissue necrosis much greater than skin necrosis. 3 , 4 , 5
Although excess or localized pressure remains the center of this problem, other contributing factors should not be ignored. These include shearing forces, which may worsen superficial damage, moisture (usually from bladder or bowel incontinence), which may hasten skin breakdown, and friction (usually from patient transfers), which may tear skin. Other factors that contribute to poor wound healing similarly affect pressure ulcers. Considerations such as poor nutrition, underlying infection, chronic edema, and peripheral vasculature disease can increase the time or resources necessary for wound healing. 6 , 7
Several recent studies have outlined risk factors such as elderly age, male gender, long-term admission, history of ulcers, diabetes, and falls. Bedbound status, poor nutrition, and a prior stroke also contribute in addition to lymphopenia, dry sacral skin, low weight, high illness severity scores, and residents of nursing homes. In these patients, it is crucial to balance prevention efforts with the level of risk. 8 , 9 , 10 , 11 , 12 , 13
Both the Norton scale and Braden scale can be used with 70 to 90% sensitivity to identify those patients at risk for pressure ulcer formation 14 , 15 The Norton scale uses mental and physical condition, activity level, mobility, and incontinence factors in its formula, while the Braden scale focuses on sensory perception, moisture level, activity, mobility, nutritional status, friction, and shear force. 15 , 16 However, evidence supports that good clinical judgment can be equally as effective as a risk predictor. 17 , 18
The diagnosis of pressure ulcers is largely clinical, with early recognition of pressure ulcers allowing for early treatment. Grading of pressure ulcers follows the National Pressure Ulcer Advisory Panel Staging System. The original staging system developed by Shea in 1975 was revised in 2007 by the National Pressure Ulcer Advisory Panel. The panel stages pressure ulcers by six categories: stages I, II, III, IV, unstageable, and suspected deep tissue injury as described in Table 11‑1. 19
Lastly, many patients will present with acute or chronic soft-tissue infection, colonization, or underlying osteomyelitis. In these patients, infection control is paramount to reconstructive interventions.
11.3 Preparation for Surgery
Prior to surgical intervention, it is essential to have an in-depth discussion with the patient regarding postoperative expectations and outcomes. Traditionally, flaps for pressure wounds necessitate prolonged bed-bound status, maintenance of nutritional intake, and other aspects of wound care which may require significant patient cooperation. Given the limited number of wound coverage options, it is imperative to optimize chances for flap success. This frequently requires a fully informed and well-prepared patient prior to surgical intervention.
Before reconstruction can take place, the site must be free of infectious nidus. This typically involves soft-tissue debridement with potential extension to bone. Flap viability is severely compromised in the setting of high bacterial growth. 20 In that respect, deep wound cultures should be taken to tailor antibiotic therapy. In the setting of suspected osteomyelitis, magnetic resonance imaging (MRI) and bone biopsy may be used for diagnosis and further tailoring of a prolonged antibiotic course. If underlying osteomyelitis is not treated, flap failure may result.
In addition to control of local infection, optimization of nutrition is crucial to promote normal wound healing. Adequate sources of protein (1.5–3g/kg/day) and nonprotein calories (25–35 cal/kg/day), as well as vitamins and minerals, should be obtained. 21 Nutritional markers such as albumin and prealbumin may be warranted to trend progress, which should be balanced with timing of optimal wound reconstruction.
Diabetes plays an important role in wound healing; hemoglobin A1c greater than 6 has been associated with wound dehiscence and recurrence. 22 Additional factors such as smoking cessation and cardiac risk mitigation should also be discussed with the patient.
Preoperative planning for moisture control should also be considered. Fecal incontinence introduces high moisture, bacterial load, and shearing forces during routine cleaning. While this can sometimes be controlled with local hygiene, fecal diversion via colostomy may be necessary. If urinary incontinence is an issue, then bladder catheterization may be indicated as well.
Generally, it is believed that enzymatic debridement with the use of products such as collagenase, papain, or urea can be used for devitalized tissue in stage I and II pressure ulcers. Many chemical solutions have been used including Dakin’s solution, hydrogen peroxide, and iodine to assist with mechanical debridement of devitalized tissue, but should otherwise be used with caution. 20 These agents are effective in controlling bacterial load, but also may be detrimental to human cells needed for healing. Mechanical and surgical debridement is generally recommended for decubitus ulcers stage III or higher.
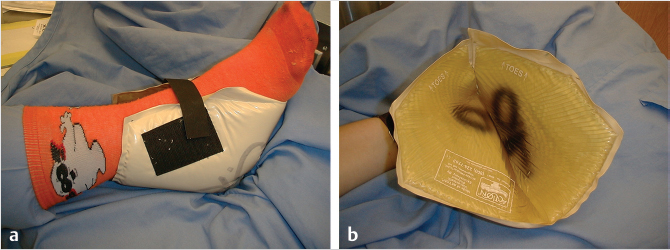
Despite all operative and ancillary care, surgical reconstruction is of little benefit without plans for future prevention, most importantly pressure relief. In the immediate postoperative period, flap healing is compromised in the setting of ischemic tissue promoted by high pressures; so, plans for support services, mattresses, and cushions must be arranged preoperatively (Fig. 11‑5; Fig. 11‑6; Fig. 11‑7).



Furthermore, without sufficient health literacy and social support, many patients are unable to continue to provide themselves with these environments, resulting in development of new pressure wounds. In that sense, coordinated efforts should be made to provide continued assessment, education, and care for these patients.
11.4 Treatment
11.4.1 Indications for Surgical Intervention
The decision to proceed with surgical intervention for pressure ulcers varies with the specific circumstances of the patient and the surgical team involved. It is important that the patient be optimized from a medical standpoint, as discussed previously. Control of infection with appropriate antibiotics and tissue debridement and optimization of nutrition are necessary. 23 , 24 . Generally, a serum prealbumin of greater than 15 mg/dL is considered within the normal range and would represent suitability for surgical intervention. Likewise, factors that created the pressure ulcer should be resolved: ischial pressure ulcers are often formed in the seated position, being caused commonly in the wheelchair bound patient. Patients can often identify a change in brand of cushion, wheelchair, or device that caused the formation of the ulcer. It is important to correct these factors as to not cause breakdown postoperatively. Lastly, social hurdles that may prevent the patient from succeeding in flap surgery must be identified. Lack of resources for special equipment including beds and wheelchairs, as well as lack of social support for long-term care, can hinder the patient’s recovery and overall success postoperatively. 20 Due to the magnitude of the surgery, the resources required, and the high risk of recurrence, a patient should have been medically optimized and have failed all conservative nonsurgical treatments prior to proceeding into surgical reconstruction. In addition, they should understand the long-term recovery associated with flap reconstruction, need for life-long compliance, and have resources in place prior to proceeding with reconstructive or flap surgery.
11.4.2 Operative Interventions
Surgical intervention can be largely divided into debridement and reconstruction. In most cases, both are required for a successful outcome.
11.5 Debridement
Operative debridement of pressure sores has several key goals. First and foremost begins with removal of necrotic, dead areas as well as chronic scar. This will enable better wound care, including use of enzymatic debridement application, as well as placement of vacuum-assisted closure (VAC) therapy. Second, debridement should remove or control soft tissue and bony infection. Removal of all infected tissues improves chances of success by minimizing bacterial load and biofilms within the wound bed, as these will both impede wound healing and potentiate failure of flap reconstruction. It is recommended that tissue be sent for pathology and culture as to help narrow antibiotic choice postoperatively. Removal of necrotic bone reduces bacterial burden, while also eliminating the bony prominence that was the causative pressure point. Debridement should be performed until healthy bleeding tissue is present in the wound bed. Likewise means of controlling the significant bleeding which is present in chronic wounds, such as sutures and electrocautery, should be readily available. Debridement of small pressure sores is possible at bedside in insensate tissue. However, debridement should ideally be performed in the operating room for large wounds with extensive tissue necrosis, tunneling, and tracking.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


