Key Words
checklist, algorithm, quality, safety, WHO, outcome, process, safety
Synopsis
Surgery requires orchestration of numerous components, including requirements for satisfactory operating space; a clean, safe environment; working sterile equipment; and qualified anesthesia, nursing, and theater personnel. Also essential are factors outside of direct perioperative control. Guaranteeing that all of these pieces come together in the correct sequence, with the right timing, for every case is difficult under the best of circumstances. In austere operating environments, achieving these goals can be difficult at best. To facilitate a systematic approach to these myriad issues with the goal of improved safety and desirable outcomes, perioperative personnel including surgeons, anesthesiologists, and nurses rely increasingly on a variety of processes and protocols to help drive the proper and safe completion of these tasks. The most prominent of these to date is the World Health Organization (WHO) Safe Surgery Checklist, but other checklists are used increasingly.
Measuring Quality
The measure of quality in medicine in general and surgery specifically is a relatively new field. The importance of measuring quality is generally first attributed to Donabedian. First published in 1966, the concept emphasized the importance of quality, which he divided into structure, process, and outcome measures. Though modified by several researchers over the decades, these three foundations still serve as a framework for approaching myriad issues that continue to stand in the way of delivering high-quality, safe surgical procedures. More recently, research in high-income countries has shown that medical errors contribute to a significant number of poor patient outcomes. The incidence of errors in poorly resourced environments is less well known, but may be presumed to be high as well, if not higher. These poor outcomes and the errors that lead to them occur despite the presence of altruistic health care providers who often work in sub-optimal environments. In highly resourced countries, these errors and the subsequent outcomes have driven many changes in the way health care is delivered. Though grounded in a quest for improved patient safety, these initiatives have a large financial component as well, because health care is reimbursed by both federal and private entities. The possibility of a reduction of errors, and the concomitant financial savings, is a large driver for the quest to improve quality and reduce patient errors. This chapter will explore ways to assess quality, methods that have been used to date to improve upon problem areas, and approaches to applying these solutions to the delivery of surgical care in more poorly resourced environments.
Structural Issues Affecting Quality
Multiple structural issues affect the quality of care delivered in the perioperative arena, in part because surgery is so resource intensive. These issues include the soundness of the facility itself and infrastructure issues such as the availability of clean operating theaters with working lights, a functional operating table, adequate suction, and a reliable oxygen source. Often, a backup generator is required due to the unreliability of supplied power. Sterilizing equipment, surgical instruments in good condition, and working anesthetizing equipment must all be available for an operation to proceed. In addition, proper instruments that are in good repair must be assembled for a specific case (case cart) and be available in a timely fashion. Personnel requirements contribute to structural requirements for quality as well, from availability of a surgeon to the presence of a qualified scrub tech for the passing of instruments. Indeed, a complete team is necessary for all but the most rudimentary of surgical procedures. Other structural components outside of the theater but equally important include the availability of a working, staffed recovery area, a bed for the patient to move to after immediate post-operative recovery, and ancillary services that may be required, such as a blood bank, an x-ray machine, ventilator, or intensive care unit. Ensuring that all of these structural quality measures are in place is a major, expensive undertaking in the best of circumstances; in a limited environment, a deficiency in any one of these can be the contributor to a poor outcome.
Process Issues Affecting Quality
Whereas structural quality measures typically have a physical component, either a thing or a person, process measures do not. Rather, they represent a series of steps that have been developed in response to a real or perceived deficiency in quality, in an attempt to improve patients’ outcomes on a consistent basis in a uniform way. Process and outcome measures of quality may be confused. Process measures represent a method, whereas outcome measures, discussed more fully later, represent the result of one or more of the methods used. Processes are sometimes referred to as outcomes but in reality are a surrogate for a real outcome or result. To improve quality, many processes have been developed. Perhaps the most well-known was the introduction of the World Health Organization (WHO) 19-item Surgical Safety Checklist. What is important to understand is that the checklist represents a method. The question incumbent upon a provider or institution that has initiated this or any other process is whether it has had the desired effect, be that improving clinical care, financial impact, and so on.
Outcomes Studies Related to Process Improvement
A brief discussion on outcomes is warranted because they should be the drivers of which processes are kept and which are replaced. Outcomes are the results of specific or non-specific processes. A well-designed study might measure the rate of surgical site infection before and after the introduction of a standardized process for ensuring the administration of prophylactic antibiotics before incision in those cases where antibiotics are indicated. Before introduction of the standardized process, there may have been administration of antibiotics in sporadic cases, in a non-standardized way. After initiation of the process, the outcome surgical site infection can be compared pre versus post the intervention process: a uniform method to address the need for prophylactic antibiotics before incision for every case. In theory, it should be relatively easy to decide whether a process is helpful in producing a desired outcome, but that is often not the case. To measure true outcome differences, well-designed randomized controlled trials are required, preferably double-blinded. Outcome differences are often uncommon enough that a large number of study patients, the study’s power, is required to show a meaningful difference between the control and intervention groups. This may require that the study be conducted across a large number of institutions. The study must control for a variety of patient characteristics, confounding variables, which is often difficult. Outcome differences found in well-controlled studies may or may not apply to the real-world clinical situations in which clinicians practice, or to the population of patients or locations in which a clinician practices. In other words, it may be difficult to generalize the results of the study, even if it has been conducted in a rigorous fashion. Finally, conducting studies is expensive and takes precious clinical time away from health care providers who may not have the resources for research, especially in the developing world. Nonetheless, whenever possible, outcomes are and should continue to be the gold standard against which the efficacy of processes are judged. Other ways that clinicians examine the efficacy of processes is through the use of clinical registries, systemic reviews, and meta-analyses.
An example of an outcome study applied to a process is that of the WHO’s Safe Surgery Saves Lives Surgical Safety Checklist. The use of a structured process was evaluated at eight hospitals representing a variety of economic environments and patient populations. In a before-after design, the study evaluated the occurrence of the primary outcome of death occurring within 30 days of surgery. Secondary outcomes were those defined as a major complication in the American College of Surgeons’ National Surgical Quality Improvement Program. Note that the checklist included a very important structural piece to this process, the use of pulse oximetry. Before the formalization of the process, most of the hospitals had variable pieces of the process in place (i.e., they had non-standardized processes). The before-after intervention involved 3733/3955 patients, respectively, and showed a drop in complication rate from 11.0% to 7.0% after the introduction of the checklist. The death rate dropped from 1.5% to 0.8%. Both of these were statistically significant.
In a more recent study, which looked at the long-term effectiveness of use of the checklist including the use of pulse oximetry, 20 months after adoption of the checklist, researchers demonstrated a continued drop in the complication rate, by 30.7%, again significant. Furthermore, surgical site infection rate decreased 40.4%.
Finally, a meta-analysis applied to this topic evaluated 723 potentially relevant papers, narrowed to nine, then six, studies. These researchers’ results suggest the validity of the findings of a reduction in mortality and complication rate, although the small number of studies examined decreased the power of the analysis in part because of the variability in effect found from the different studies. Perhaps as interesting as the finding of the importance of the use of the checklist was the finding of the value of team compliance in using the checklist. As the authors point out, “Haynes and colleagues showed that improvements in post-operative outcomes were associated with improved perception of teamwork and safety climate among respondents, suggesting that changes in these aspects may be partially responsible for the effect of the checklist.”
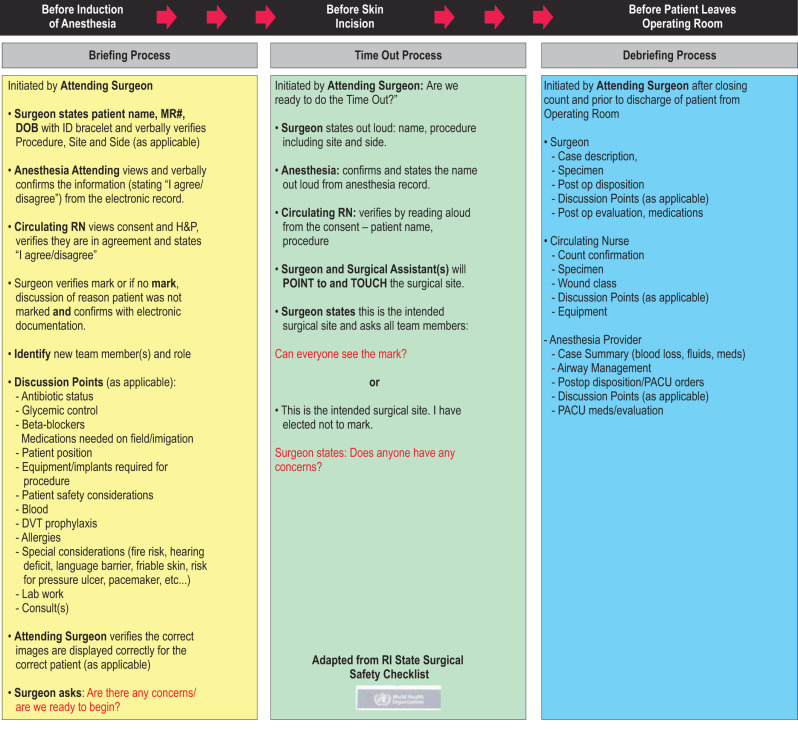
Components of the WHO Safe Surgery Checklist
It is important to point out that the WHO Safe Surgery Checklist has several components, all of which are important to undertake in a collaborative fashion between surgery, anesthesia, nursing, and other staff in the operating room. “Sign in” functions include patient identification concerns including identity, procedure to be performed, surgical site, and side. They include review of allergies, airway-related concerns, and confirming the use of working pulse oximetry. Note that the “time out” portion involves confirmation of patient identity (intentional redundancy), determination of need for prophylactic antibiotics, and communication of any concerns by each of the triad of perioperative care: surgery, anesthesia, and nursing. Finally, the “sign out” portion allows critical review of issues and discussion of patient disposition. All of these pieces promote communication before, during, and after the case, giving all parties parity, the importance of which cannot be overstressed. Innumerable examples exist of operating room mishaps because nursing or anesthesia did not feel empowered to communicate their concerns to the surgeon. It is incumbent on the surgeon to foster this atmosphere of open communication. The Surgical Safety Checklist in use at the author’s hospital can be seen in Fig. 1.5.1 . Table 1.5.1 details the checklist elements, utilized in 50 or more operating rooms system-wide for every case, every day of the year.