Key Words
general anesthesia, anesthesia delivery systems, patient monitoring, anesthesia supplies, anesthetic agents, airway management
Synopsis
Delivery of general anesthesia requires a trained anesthesia provider; the availability of functioning, safe anesthetic equipment and patient monitors; and the essential anesthetic and resuscitative medications. Anesthesia is an essential component of surgery, and when anesthesia services are inadequate, difficulties are experienced. Maintaining the safety of patients while treating them in areas with limited resources is a continuing challenge.
Minimum requirements for general anesthesia in developed countries include a source of pressurized oxygen; an effective suction device; standard American Society of Anesthesiologists (ASA) monitors, including heart rate, blood pressure, electrocardiogram (ECG), pulse oximetry, capnography, and temperature; and inspired and exhaled concentrations of oxygen and applicable anesthetic agents.
In low- to middle-income countries (LMICs), due to large economic inequities, extreme variations exist in the availability of both anesthesia providers and the necessary equipment and drugs. The provision of general anesthesia relies heavily on technology and sophisticated equipment and supplies. Often in LMICs, there are shortages of needed drugs and essential equipment (anesthesia delivery machines, monitors, laryngoscopes, and disposables such as airway devices), and for much of the anesthesia equipment donated, there are no hospital personnel capable of providing maintenance. Current practice for provision of anesthesia for reconstructive surgical procedures must be adapted to the availability of supplies and experienced anesthesia providers on-site.
General Anesthesia in LMICs
Currently, in developing countries, general anesthesia with spontaneous ventilation is the most common technique used to facilitate surgical procedures, with regional anesthesia (spinal, peripheral nerve block, or local infiltration) with or without sedation being a close second method. Provision of general anesthesia without intubation or deep sedation is often used to accommodate minor surgical procedures and wound closures. Successful training of anesthesia providers (either physicians or nurses) requires a hospital setting that has sufficient volume and diversity of operations, non-obsolete anesthesia equipment, and a structured and comprehensive training program that is recognized by the national ministry of health or other relevant professional bodies.
Anesthesia Delivery Systems (Machines, Vaporizers, and Monitors)
The most common type of anesthetic machine in use in developed countries is the continuous-flow anesthetic machine, which is designed to provide an accurate and continuous supply of medical gases (oxygen, air, nitrous oxide), mixed with an accurate concentration of anesthetic vapor that is delivered to the patient at a set pressure and flow. Availability of functional anesthesia equipment is problematic in the LMICs, with variation seen within and between hospitals. Donated equipment is often outdated and obsolete, the local providers are often not properly trained to use or repair it, and they are unable to acquire replacement parts when needed. Many anesthesia machines currently encountered in LMICs have been modified by the local providers using the only parts available, which may be non-standard and often do not meet biomedical standards. Caution must be taken when using this equipment.
Of the anesthesia machines available in LMICs, many are considered obsolete because they lack certain safety features such as oxygen monitors that display O 2 concentration, and oxygen supply pressure failure alarms or fail-safe delivery devices that would shut off gas flow and sound an alarm if a hypoxic gas mixture were inadvertently being delivered. Many also lack calibrated anesthetic vaporizers for safer volatile anesthetic agents such as isoflurane and sevoflurane, a vaporizer Pin Index Safety System and interlock device (an interlock mechanism that prevents gases from more than one vaporizer being put to use at the same time, thus causing an accidental overdose), or Diameter Index Safety System (DISS); this system consists of non-interchangeable gas line connectors that provide a standard for non-interchangeable, removable connections for use with medical gases ( Fig. 1.3.1 ).

Draw-over anesthesia machines are currently the most prevalent machines used in LMICs. They are generally portable and easy to assemble, consist of a low-resistance breathing circuit with a one-way valve to prevent rebreathing, a method to ventilate the patient such as a bellows or self-inflating bag, and a draw-over (low resistance) variable bypass vaporizer. With this type of system, the carrier gas (room air or supplemental oxygen) is drawn over the vaporizer either by ventilation supplied by the anesthesia provider (via self-inflating bag or bellows) or by the patient’s spontaneous breathing. With a draw-over vaporizer, the final oxygen concentration delivered to the patient is dependent on both the added flow of oxygen and the minute ventilation volume (respiratory rate and tidal volume) as well as on the pattern of ventilation. These vaporizers are at high risk for delivery of a hypoxic mixture.
Plenum variable bypass vaporizers, which have a much higher internal resistance and require fresh gas flow above atmospheric pressure. They are unidirectional, agent specific, and more accurate in delivery of set anesthetic concentration than draw-over type. They have become more prevalent in the major LMIC cities. These vaporizers, which can produce a more accurate concentration of agent at very low gas flows, are similar to those seen in industrialized countries. Most vaporizers encountered in LMICs, when available, are often not properly calibrated, risking potential for the delivery of erroneous concentrations of an inhalational anesthetic agent. Recently more LMIC hospitals have been able to acquire sevoflurane vaporizers; however, the majority of sites in the rural areas still make use of halothane, isoflurane, enflurane, and ether vaporizers ( Fig. 1.3.2 ).

Measured-flow vaporizers are obsolete in the United States; however, they may still be encountered in the form of the Copper Kettle, Verni-trol, Metomatic, and Boyle Bottle and Goldman vaporizers in LMICs ( Figs. 1.3.3 and 1.3.4 ).


The concentration of anesthetic delivered with these devices is dependent on the vapor pressure of the anesthetic liquid, the gas flow through the device, and total gas flow in the system. When delivering halothane via a measured-flow vaporizer, the typical flow rate to the vaporizer is set at 100 mL/min and the fresh gas flow at 5 L/min, which gives a concentration of approximately 1%. With these delivery systems, it is critical to ensure sufficient diluent gas to prevent a lethal dose of halothane being delivered to the patient. Halothane and, to a lesser extent, ether are volatile anesthetics commonly used in developing countries. Ether is an excellent analgesic that is still used in LMICs due to its low cost and its relative safety, because it does not depress respiration or the cardiovascular system. Disadvantages seen with this anesthetic agent are that it has extremely high lipid solubility, leading to very slow onset and slow emergence, and it is very pungent, making it difficult to use for induction. It is also associated with a high incidence of post-operative nausea and vomiting (PONV) and is extremely flammable and occasionally explosive in oxygen. Ether use is now limited due to decreased availability and flammability.
Halothane has been replaced by sevoflurane in the operating rooms of most developed countries and is no longer available in the United States. As a result of this lack of demand and absence of profit, pharmaceutical companies selling this product are threatening to stop production, which could be a threat to the hundreds of thousands of patients in LMICs who are dependent on this anesthetic for surgical procedures. Halothane, like ether, is inexpensive and is still used for both mask induction and maintenance anesthesia. This agent, in comparison with newer agents such as isoflurane and sevoflurane, has an increased risk of sensitizing the myocardium to exogenous epinephrine, which commonly results in dysrhythmias such as junctional rhythm, bradycardia, pre-ventricular contractions, or ventricular tachycardia. Complications when using halothane frequently arise during mask induction of anesthesia or during surgical infiltration of tissues with local anesthetic containing epinephrine.
Halothane may be delivered from an isoflurane vaporizer and vice versa because the two agents have very similar vapor pressures. If doing so, care must be taken to completely empty vaporizers before filling to avoid delivery of a gas admixture. One must be extremely cautious if delivering halothane via an isoflurane vaporizer because it has the potential to deliver up to a 5% concentration of halothane.
Soda lime carbon dioxide scrubbers present in local LMIC hospital anesthesia systems may be old or exhausted and may not change color to signal when patients develop hypercarbia. If soda lime is unavailable, a patient’s Pa co 2 may be better controlled with a non-rebreathing circuit, such as a Mapleson D or Bain circuit. Rebreathing with these circuits can be avoided and normocarbia maintained by keeping the fresh gas flow high at 1.5 to 2 times per minute ventilation. Suggested fresh gas flow with the use of a Mapleson D system or Bain circuit is 200 to 300 mL/kg with spontaneous ventilation, 2 L/min fresh gas flow in patients <10 kg, 3.5 L/min fresh gas flow in patients 10 to 50 kg, and 70 mL/kg fresh gas flow in patients >60 kg during controlled ventilation. The disadvantage of non-rebreathing systems is that they require large fresh gas flows that may rapidly deplete available oxygen supplies.
Anesthetic ventilators, taken for granted in developed countries, may be available in some LMIC centers; however, they often are not serviced, leading to delivery of inappropriate tidal volumes and presenting risk of barotrauma.
Volunteer surgical service organizations often transport the equipment, monitors, and supplies needed to provide general anesthesia for short-term surgical missions; however, they still must rely on in-country electricity, water, and oxygen supplies, which are often intermittently unavailable at most sites, or permanently unavailable at some of the rural LMIC sites. In hospitals in developed countries, the primary gas source for the anesthesia machine is a pipeline supply source delivered through wall outlets at a pressure of 50 to 55 psig. In most LMIC hospitals, the oxygen source is typically supplied in tanks. When oxygen is available from a wall outlet, it is likely that the line is connected to large oxygen tanks outside the hospital and not the typical liquid oxygen reservoirs used in developed countries. Oxygen tank size and color code also vary according to location. US standards require oxygen tanks to be green, whereas the World Health Organization (WHO) specifies that they be white. The most common tank cylinders available are type E, G, or H. The E cylinders contain 625 L of oxygen, corresponding to a pressure of 2200 psi. The G and H cylinders are much larger and can hold 5300 L and 6900 L of oxygen, respectively, when completely full. When oxygen supply to an anesthesia machine is by tank, one should always have a backup tank on-site and immediately available. Due to the cost and limited availability of the oxygen supply, whenever possible, the fresh gas flow used to deliver an anesthetic should be minimal (1–2 L/min), and providers should turn off flows when not in use.
In some rural hospitals, there is no available source of oxygen, and providers are dependent on oxygen concentrators. These machines run atmospheric air through zeolite, which absorbs nitrogen, to produce an admixture that is 95% oxygen concentration.
Other gases such as nitrous oxide are often not available. However, when they are being used, one must be vigilant to frequently check the oxygen supply source and to continuously monitor patient oxygen saturation, because delivery of a hypoxic gas mixture can easily occur if the oxygen source is empty. This is especially true if safety devices such as proportioning systems and the measurement of inspired oxygen concentration are not present.
Waste gases emitted from the anesthesia machine can be detrimental to operating room personnel when inhaled. In developed countries, these gases are scavenged to a central vacuum system or to a passive duct system that safely transports the waste gases into the atmosphere. Often in LMIC operating rooms, these gases are not scavenged, and they are released directly into the operating room. They can easily be scavenged from anesthesia machines by running corrugated tubing from the exhaust valve of the breathing system to an outside window or a suction device.
The WHO recommends that the minimum standard of care for patient monitoring while receiving anesthesia consists of pulse oximetry, heart rate monitoring, non-invasive blood pressure recording, and temperature monitoring. It also suggests monitoring the capability for inspired and exhaled concentrations of oxygen and applicable anesthetic agents and also monitoring the availability of additional equipment such as bag valve masks, laryngoscopes, oral airways, precordial stethoscopes, and cricothyrotomy kits.
The patient monitors encountered in LMICs are often suboptimal, with missing or broken parts and cables, or none at all. In most facilities, there are no volatile anesthetic or EtCO 2 gas analyzers, and the ability to monitor ECG and pulse oximetry is also sporadic. Often, anesthesia providers must rely on obtaining blood pressure via blood pressure cuff and sphygmomanometer and auscultation of breath and heart sounds with a precordial stethoscope. In some rural areas, monitoring may consist only of a precordial stethoscope and the vigilance of an anesthesia provider with a “finger on the pulse.”
Pulse oximetry was recognized as an international standard in anesthetic care in 2009, and it is the only piece of technological equipment required by the WHO Surgical Safety Checklist.
Temperature monitoring is often not available in LMICs. Temperature monitoring should be utilized for cases in which the patient is at risk for significant hypothermia, which may be seen during procedures requiring large body portions to be exposed, or where blood loss with repletion may be necessary. Temperature monitoring may also be needed for patients having procedures in warmer climates where operating rooms have no air conditioning systems, because these patients are at risk for hyperthermia.
A continuous source of electricity is needed to power most anesthesia equipment including monitors and ventilators. Anesthesia providers in LMICs must be prepared for frequent power outages. If possible, a backup generator should be available. The anesthesiologist, surgeon, and nurses should have backup plans for how to monitor the patient’s vital signs and how to provide light, suction, and hemostasis during power failure. Equipment brought by teams should have a backup rechargeable battery source. Because the electric power source current may differ from that in the United States, current converters, plug adapters, and grounding devices may be needed.
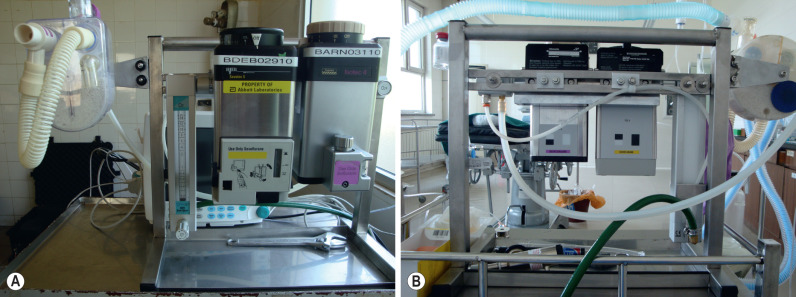
Volunteer surgical teams may consider transporting portable anesthesia machines; however this requires knowledge of how to set up and troubleshoot them. Machines that are brought must have gas connection hoses with connected fittings that have the capacity to attach to the oxygen gas cylinder valve outlets and pressure regulators at the host sites, and the machines will also need appropriate tubing that enables waste gases to be disposed into the atmosphere. Figs. 1.3.5A and 1.3.5B depict a portable anesthesia machine utilized by ReSurge International. This system contains a stand that holds oxygen tubing with connectors from tank pressure regulators to a flow meter; to temperature-compensated, concentration-calibrated, dial-controlled sevoflurane and isoflurane vaporizers; and to a portable baralyme circle system (“King System”) ( Figs. 1.3.5A and 1.3.5B ).
Anesthetic Disposable Supplies and Medications in LMICs
Most anesthetic supplies that are considered “single-use disposables” in the United States are cleaned and reused in LMICs. Sterilization practices are varied, and often inadequate, with increased risk of iatrogenic infections. Pediatric-size endotracheal tubes (ETTs) are extremely limited and often unavailable. Available supplies are recycled numerous times, which puts them at risk for weakening, kinking, and balloon cuff rupture. Pediatric anesthesia circuits, masks, oral airways, laryngeal mask airways (LMAs), and intravenous catheters are a rare commodity.
When reusing supplies, careful cleaning and disinfecting processes should be followed. Laryngoscopes, ETTs, suction catheters, oral airways, LMAs, masks, and other equipment exposed to mucous membranes and bodily fluids should first be thoroughly washed with soap and water to remove particulate organic matter. After initial cleaning, it is then advisable to soak the equipment in a high-level chemical disinfectant or use a sterilization process. Examples of high-level disinfectants include glutaraldehyde 2% to 3.5% (Cidex ® ), ortho-pthalaldehyde (Cidex-OPA ® ), sodium hypochlorite 1000 to 2500 ppm (bleach), hydrogen peroxide 6%, iodine at a concentration of 450 ppm, and 70% to 90% ethyl and isopropyl alcohol. These disinfectants are bactericidal, tuberculocidal, fungicidal, and virucidal with 10- to 40-min exposure. Steam sterilization, if available, can also be used on plastic disposables once washed, but repeated treatments tend to discolor and weaken the plastic. Any equipment that has been washed should be completely dry before reuse.
Hospitals in LMICs frequently have poorly organized storage and distribution of health care–related disposable products and drugs. Often stock supply levels are unknown, and a continuous supply of disposables and essential drugs is not reliable. Many anesthetic and resuscitation medications that are standardly stocked in operating room pharmacies in the developed countries may be unavailable in LMICs. It is vitally important to check all drug labels for the concentration before administering, because drug concentrations found abroad may differ from the standard concentrations seen in the United States. When diluting medications to a certain concentration, a standard dilution should be chosen and used for every case as a measure to avoid drug-dosing error.
Surgical teams should create a list of the names and amounts of medications required to provide anesthesia for the number of expected cases, and specific to the procedures being performed. When general anesthesia is being performed, this usually consists of premedications, induction agents, analgesics, volatile anesthetics, muscle relaxants, local anesthetics, antibiotics, anti-nausea medications, and drugs required for resuscitation.
When preparing and packing medications and disposable supplies for a surgical trip, it is wise to consider bringing anything thought to be essential for providing safe general anesthesia. Packing lists will vary depending on the number and type of surgical procedures being performed. Box 1.3.1 is an example of an anesthesia supply list of items necessary for a plastic reconstructive surgical mission.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


