The pedicled anterolateral thigh flap is a useful addition to our armamentarium. It provides excellent cover for defects in the lower abdomen, pelvis, and perineum. It also has the added advantage of not sacrificing any muscle, thereby minimizing the risk for donor morbidity. This article reviews the major applications of the proximally pedicled anterolateral thigh flap, describes the technique of flap harvest, and discusses techniques of flap transposition as well as pointing out some potential hazards.
Since it was first described by Song and colleagues in 1984, the anterolateral thigh flap has been more commonly used as a free flap than as a pedicled flap. However, it is extremely useful as a pedicled flap and can be used to reconstruct a wide variety of defects in the pelvis, the perineum, and the lower abdomen. For these purposes, the flap is pedicled on proximal flow from the descending branch of the lateral circumflex femoral artery. Distally based pedicled anterolateral thigh flaps are described but are not discussed other than to caution that venous outflow can sometimes be a problem with this particular configuration. However, they have been used successfully in the coverage of defects around the knee and the lower leg. Here the authors describe the use of the proximally based anterolateral thigh flap for reconstruction of perineal, pelvic, and lower abdominal defects. This article reviews the major applications of the proximally pedicled anterolateral thigh flap, describes the technique of flap harvest, and discusses techniques for flap transposition as well as pointing out some potential hazards.
Vascular anatomy
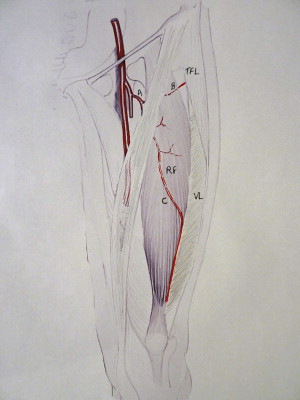
The vascular anatomy of the anterolateral thigh flap has been well described. It is important to note, however, that one side of the body is not a mirror image of the other and, as with other perforator flaps, a case can be made for preoperative imaging. The blood supply comes from the descending branch of the lateral circumflex femoral artery. An ascending or transverse branch supplies the tensor fascia lata muscle and the skin overlying that muscle. The descending branch runs between vastus lateralis laterally and rectus femoris medially. The overlying skin is supplied, for the most part, by intramuscular perforators that usually run through vastus lateralis and less frequently through rectus femoris. Perforators supplying the flap usually penetrate the anterior aspect of the vastus lateralis ( Fig. 1 ). In less than 15% of cases, the perforators run in the septum between the 2 muscles. In this situation no intramuscular dissection is required. The configuration of the perforators has been described by Yu and Youssef. They describe A, B, and C perforators, with A being proximal and C distal to perforator B. The nerve to vastus lateralis runs alongside the main pedicle. Care must be taken during dissection to ensure that the nerve is not injured.
Flap design
A line is drawn from the anterior superior iliac spine to the lateral border of the patella ( Fig. 2 ). This line represents the surface marking of the septum between vastus lateralis and rectus femoris. The midportion of this line marks the site at which the perforators are most likely to be encountered and detected. The authors’ preference is to use a hand-held Doppler to locate the perforators, recognizing that this method may not always be accurate. The flap can be raised to include any of the elements supplied by the vasculature. It can incorporate muscle (vastus lateralis), fascia, and skin. The choice of which tissues to include will be dictated by the reconstructive requirements. The technique may be modified accordingly. For many of the reconstructive applications that a pedicled anterolateral thigh flap can address in the lower abdomen, the fascial element of the flap can be important, which is particularly the case when reconstructing through abdominal wall defects. Often, the amount of fascia required is larger than the amount of skin required. If this is the case, an excess of fascia over skin can easily be harvested ( Fig. 3 ). Vascularized fascia lata in abdominal wall reconstruction is said to have the advantage of preventing adhes between the fascia and the abdominal viscera. If no fascia is required for the reconstruction, then a skin-only flap can be designed and the fascia simply incised around the perforators ( Fig. 4 ). Furthermore, if muscle is a required element of the reconstruction, the flap can be raised as a myocutaneous flap incorporating the vastus lateralis muscle. The technique of dissection will depend on what elements are being included with the flap. The dimensions of the flap will obviously be dictated by the size of the defect to be reconstructed. However, the vascular pedicle of the anterolateral thigh can carry a large flap (up to 30 cm). To perfuse such a large skin paddle, however, more than 1 perforator may need to be harvested with the flap. If multiple perforators are available, it is judicious to sequentially clamp them so as to ensure that the selected perforators will perfuse the flap (see Fig. 4 ). Pedicle length can also be particularly important when the flap is being designed as a pedicled flap; the longer the pedicle, the greater the arc of rotation. Preoperative imaging may be particularly helpful when planning a pedicled anterolateral thigh flap because the location of the perforator has a bearing on pedicle length and, therefore, on the arc of rotation of the flap. A distally placed perforator, the C perforator according to Yu’s classification, can add considerable length and can be chosen if it is of appropriate size. The more distal perforators, however, tend to have a longer intramuscular course. Although the extra pedicle length gained from dissecting these perforators may be desirable, the amount of intramuscular dissection can be an important issue. Regardless of the position of the perforator, size is important and the perforator needs clinical evaluation to ensure that it can adequately perfuse the flap. As already mentioned, if ever there is any doubt, sequentially clamping the perforators (see Fig. 4 ) can be a good way to determine which perforator offers the best perfusion.
The width of the flap is also important because it will determine whether or not the donor site will need a skin graft or whether it can be closed by direct approximation. Direct closure is desirable because a skin graft in this area is unsightly and not always well tolerated by patients. Although it is generally accepted that a width of 8 cm can usually be closed directly, it has been the authors’ experience that much wider defects can be closed directly. If the flap does not contain fascia, it is generally much easier to close the donor defect than when the fascia has been harvested with the flap because the fascia contains and constrains the thigh musculature, which, when fascia has been harvested with the flap, tends to bulge and make closure more difficult. Regardless of whether or not fascia has been harvested with the flap, penetrating towel clamps can be used to temporarily approximate the wound edges ( Fig. 5 ) allowing sufficient tissue creep to facilitate closure. Care must be exercised, however, in situations where patients are unable to report symptoms that might indicate too tight a closure. The authors have encountered 2 cases of compartment syndrome, in the presence of epidural anesthesia, that was caused by a closure that was too tight.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


