Over the past decade, muscle perforator flaps have proven their versatility as another important option when a soft tissue flap is essential. Valuable as either local or free flaps, these are no longer a novelty, and are perhaps even becoming a necessity for the mainstream reconstructive surgeon. Prior microsurgical capabilities will unquestionably simplify the transition to harvesting the diminutive vascular pedicle of these flaps, while perhaps shortening the learning curve, but these skills are not imperative. With proper assistance and perseverance, as with any other aspect of surgery, muscle perforator flaps can become a mainstay, if not the preferred method, for soft tissue repairs even in the community hospital where resources tend to be less available.
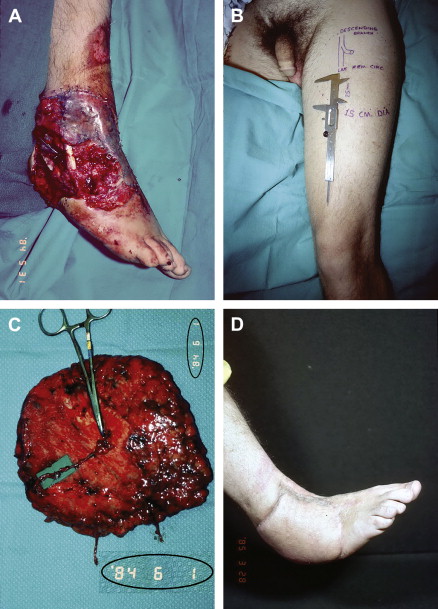
In early 1984, Song and colleagues showed how a large, undelayed fasciocutaneous flap could be reliably raised from the anterolateral thigh based on a septocutaneous perforator from the descending branch of the lateral circumflex femoral vessels. The author’s senior partner at the time coincidentally was referred a patient who had degloved his ankle and heel pad in a motorcycle accident, with exposure of the Achilles tendon and multiple open fractures of the hindfoot ( Fig. 1 ). Because of the extremely large size of the defect, he suggested that, although a novel idea, this thigh flap would be a terrific solution if used as a microsurgical transfer. The requisite huge flap was designed and raised following all of the instructions carefully; and predictably—in retrospect—no septocutaneous perforator could be found, but instead after dissection of the entire anterior thigh there was only a single, and what was considered a relatively tiny, musculocutaneous perforator of the vastus lateralis muscle. With no guidelines to follow, instead of abandoning this donor site, it seemed plausible to tediously dissect the perforator through the muscle, with careful coagulation of all muscular side branches, back to a reasonably large caliber source vessel. Despite the trepidation in doing this, the flap survived completely without further sequelae (see Fig. 1 ).
After gleaning through the original Song and colleagues article now numerous times since, a fine print disclaimer is noted that states that occasionally the perforator to what is still today called the anterolateral thigh flap may pass “through a thin layer of muscle fibers before entering the skin.” The author’s group had actually harvested a muscle perforator free flap without knowing it, because this appellation did not exist at that time. Compared with the more conventional muscle free flap donor sites in use then, this dissection had been so difficult and the stress of performing just a microvascular anastomosis was so great because the authors had just begun that learning curve that they vowed never to use this flap again. Little did they know what the future would bring.
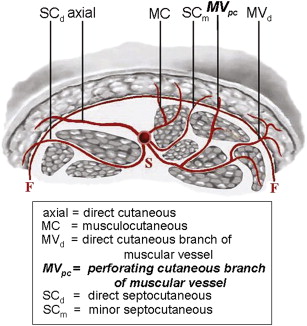
Disregarding the preceding historical footnote, the role of fasciocutaneous flaps as a soft tissue alternative or supplement to muscle flaps, which were popular at that time, became obvious and otherwise intriguing. A relatively obscure treatise in 1986 by Nakajima and colleagues suggested that the deep fascia has 6 different types of perforators, and that each could potentially nourish a skin flap ( Fig. 2 ). Although one of these, the perforating cutaneous branch of muscular vessel , traversed the muscle, its intended course was primarily directly to the integument. They postulated that this perforator could stand alone to serve a “perforating cutaneous branch of muscular vessel flap.” Because this type of flap will always require the tedious intramuscular dissection of that musculocutaneous perforator, Wei and colleagues defined these as “true” muscle perforator flaps.
The author’s personal reindoctrination into this concept of muscle perforator flaps awaited his response to a flyer advertising the 5th International Course on Perforator Flaps in Gent, Belgium in 2001, at which Steve Morris had also matriculated to be an observer. As overseen by the course chairman, Philip Blondeel, the attributes of muscle perforator flaps became more apparent, including their large potential size, large-caliber vessels with long vascular pedicles, and abundance of donor sites to better match the characteristics of any possible recipient site. In an attempt to be intimately involved in this nascent field, the author presented an abstract reviewing anatomic dissections of gastrocnemius musculocutaneous perforators just before a clinical series by Cavadas and colleagues, which is now known as the sural artery perforator flap according to the Canadian nomenclature terminology. One of the panelists, Fu Chan Wei, in response to the author’s question, actually entered the audience to debate just what were “perforator flaps.” This discussion led to the idea that perforators could be “direct” or “indirect,” with muscle perforator flaps the quintessential representative of the latter and enduring as the primary topic of that course, and for the remainder of this compendium, for the sake of clarity.
Method and materials
The author’s private practice in a community setting started after completion of typical University training in 1982. Random flaps were still in vogue, and therefore this opportunity permitted the introduction of the relatively new concept of muscle flaps, followed soon after by various forms of fasciocutaneous flaps, both proving to be a better technique for soft tissue reconstruction ( Table 1 ). Although readily transferred as local or pedicled flaps, the existing vacuum of other plausible alternatives allowed investigators to hone their microsurgical skills and enabled the simultaneous introduction of microvascular tissue transfers, or free flaps (see Table 1 ). From an awkward beginning, and thereafter often following a rocky road virtually without knowledgeable supervision, muscle perforator flaps were eventually reintegrated in 2001 (see Table 1; Table 2 ) into what has primarily been a solo practice within this same community from 1982 to now.
| Year | Fasciocutaneous | |||||
|---|---|---|---|---|---|---|
| Muscle | Perforator | Nonperforator | ||||
| Local Flap | Free Flap | Local Flap | Free Flap | Local Flap | Free Flap | |
| 1982–1986 b | 18 | 6 | 7 | 4 | ||
| 1987–1991 b | 13 | 8 | 21 | 5 | ||
| 1992–1996 b | 18 | 10 | 14 | 5 | ||
| 1997–2001 b | 32 | 18 | 13 | 4 | ||
| 2002 | 27 | 25 | 11 | 19 | 14 | 5 |
| 2003 | 34 | 30 | 5 | 6 | 14 | 4 |
| 2004 | 29 | 21 | 8 | 21 | 13 | 7 |
| 2005 | 38 | 16 | 8 | 29 | 13 | 3 |
| 2006 | 18 | 5 | 10 | 28 | 19 | 6 |
| 2007 | 18 | 10 | 11 | 27 | 16 | 4 |
| 2008 | 21 | 20 | 7 | 39 | 18 | 6 |
| Local Flap | Free Flap | Total | |
|---|---|---|---|
| Anterolateral thigh | 7 | 108 | 115 |
| DIEP | 3 | 29 | 32 |
| SAP | 16 | 15 | 31 |
| MCFAP | 7 | 19 | 26 |
| GAP | 13 | 1 | 14 |
| All others | 20 | 10 | 30 |
| 66 | 182 | 248 |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


