This article is an up-to-date overview of the potential uses and limitations of immunohistochemistry (IHC) in melanocytic lesions. The information is intended to assist dermatopathologists and dermatologists who read slides to appropriately use IHC in this setting. In addition, dermatologists who do not review microscopic slides will better understand the rationale of the pathologist when reading and interpreting the pathology report.
- •
Immunohistochemistry (IHC) should be used judiciously.
- •
In some circumstances, IHC is paramount to diagnosis.
- •
More often IHC simply provides additional information that must be weighed with the histomorphologic and clinical features to establish the most appropriate diagnosis or assist in planning patient management.
- •
Accurate interpretation relies on evaluation of appropriate staining pattern (cytoplasmic or nuclear), as well as independent and internal controls.
- •
Knowledge of the expected reactivity is required to correctly interpret immunohistochemical preparations.
IHC is based on reagent antibody binding to a target epitope/antigen in tissue sections. Binding of the antibody to the antigen in tissue is visualized through use of a second immunohistochemical reaction, usually either an immunoperoxidase or alkaline phosphatase-based system, resulting in a stained reaction product. The 2 most common systems used include the diaminobenzidine (DAB) method, resulting in a brown product, and “Fast Red” or amino-9-ethylcarbozole (AEC), alternatively giving a red reaction.
Accurate interpretation of immunohistochemical preparations requires review of independent and internal controls to ensure appropriate staining. One must remember that immunoreactivity and true antigen expression are not necessarily synonymous, and several factors can account for immunostaining without true expression, including inappropriately high antibody concentration and/or excess antigen retrieval. By contrast, false negatives can occur because of too much or too little fixation time. The pattern of staining is also crucial. For example, faint staining of the cytoplasm with a nuclear marker should not be misinterpreted as a positive reaction. A thorough understanding of the expected reactivity for all entities in the differential diagnosis is required and, similar to most studies in medicine, IHC is not perfectly sensitive or specific, requiring correlation with the clinical scenario and histomorphology.
Despite numerous reports in the literature, reliable meta-analysis of immunohistochemical data in melanocytic lesions is limited by several variables, including differences in antibody source, antigen retrieval methods, and antibody concentrations. Other variables include differences in subtype of tumors included (eg, in melanoma: nodular, metastatic, desmoplastic, and so forth) and the criteria used to define positive and negative reactions.
Despite these limitations, IHC can, at times, be an adjunct to the hematoxylin and eosin (H&E) morphology when used appropriately. Some cases will still defy classification, even with extensive IHC. This article reviews the most recent advances of IHC in melanocytic lesions and provides guidance in a series of diagnostic dilemmas.
Melanocytic markers
In addition to morphologic clues, IHC can assist in distinguishing melanocytic from nonmelanocytic lesions when the tissue of origin is uncertain. Staining with S100 was one of the first and most enduring markers for melanocytic lesions. While S100 is considered the most sensitive marker and stains the great majority of melanocytic lesions, this marker lacks specificity and stains Langerhans cells, sweat glands, nerves, Schwann cells, myoepithelial cells, adipocytes, muscle cells, chondrocytes, and their tumors. Therefore other antibodies may be necessary to confirm the melanocytic nature of S100-positive neoplasms, particularly melanoma ( Table 1 ). Although typically of high sensitivity, S100 is not always the preferred melanocytic marker in all settings. It should be used with caution for intraepithelial melanocytic proliferations of the nail matrix where sensitivity is low. Melan-A and HMB-45 (discussed below) are more sensitive in this small niche; however, S100 is still essential in identification of an invasive component, particularly when spindled.
| Antibodies | Pattern | Positive (N) |
|---|---|---|
| S100 | Nuclear/cytoplasmic staining | 93.4% (91) |
| Sox-10 | Nuclear staining | 89.7% (68) |
| MART-1 | Cytoplasmic staining | 88.8% (89) |
| MITF | Nuclear staining | 79.8% (89) |
| HMB-45 | Cytoplasmic staining | 75% (88) |
Melanoma antigen recognized by T cells (MART-1), also referred to as Melan-A, is expressed by normal melanocytes, nevi, and melanoma, but less frequently by desmoplastic malignant melanoma (DMM). In addition, macrophages may aberrantly label with MART-1 using some antigen retrieval techniques; however, the staining is weak and granular, in contrast to the strong expression in melanocytic cells. Macrophage staining may be due to passive acquisition of antigens through phagocytosis.
HMB-45 (anti-gp100), an organelle-specific, premelanosome marker, has been shown to mark only the intraepidermal and superficial dermal components of melanocytic nevi, with the exception of diffuse dermal staining in blue nevi and deep penetrating nevi. When compared with MART-1, HMB-45 has been found to have weaker and more focal staining in both primary and metastatic melanomas, and rarely reacts in DMM. Therefore, HMB-45 is specific, only rarely staining other tumors (eg, perivascular epithelioid cell tumor [PEComa]) but does not stain all melanomas. PEComas are tumors with immunophenotypic features of smooth muscle and melanocytic differentiation. While most are retroperitoneal or visceral, a subset arises in the skin. These lesions can mimic melanocytic neoplasms on routine sections and with IHC. HMB-45 is the most sensitive marker for PEComas, but Melan-A and microphthalmia transcription factor (MITF; discussed below) are also expressed in many cases. PEComas differ from melanocytic lesions by the absence of S100 expression.
MITF is responsible for the normal embryonic development of melanocytes, mast cells, cells of the retinal pigment epithelium, and osteoclasts. Immunohistochemical expression of MITF is nuclear. Reactivity is present in most melanomas, including some rare cases that do not express S100; however, a large proportion of desmoplastic and spindle-cell melanomas fail to react. MITF positivity has been reported in 88% of conventional metastatic melanomas and although this is slightly less than the number of S100-positive metastases (90%), half of the S100-negative metastases were MITF positive, suggesting possible use in combination. However, MITF is not specific, and staining has also been reported in PEComas, cellular neurothekeomas, neurofibromas, dermatofibromas, atypical fibroxanthomas (AFX), leiomyosarcomas, schwannomas, malignant peripheral nerve sheath tumors (MPNST), and dermal scars.
Similarly, Sox-10 is an alternative nuclear melanocytic marker. It is a transcription factor found in neural crest–derived cells and is crucial for specification, maturation, and maintenance of Schwann cells and melanocytes. Although Sox-10 stains Schwann cells and myoepithelial cells in addition to melanocytes, it is much more specific than S100 for melanocytic lesions and has shown equal or better sensitivity.
It is important to be aware that melanocytic lesions, particularly melanomas, can show aberrant expression of nonmelanocytic markers. Some melanomas exhibit aberrant expression with desmin, smooth muscle actin (SMA), CD138, MDM-2, synaptophysin, glial fibrillary acidic protein, CD30, CD68, carcinoembryonic antigen, and epithelial membrane antigen. Cytokeratin expression occurs in 4% to 6% of malignant melanomas; however, the staining tends to be focal and sparse. There is increased aberrant expression of epithelial-associated markers in melanoma metastases. Use of a panel of immunostains, including the aforementioned melanocytic markers, should help to prevent misdiagnosis.
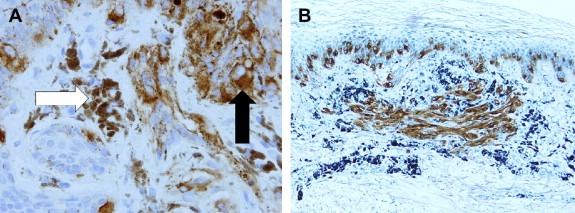
One of the problems with IHC in heavily pigmented melanocytic lesions is distinction of melanin in keratinocytes and melanophages from the brown (DAB) chromogen reaction. The color and texture of the melanin pigment are slightly different, but distinction can be cumbersome ( Fig. 1 A). One option is the use of AEC, resulting in a red product; however, this tends to smear and fade faster than DAB. Alternatively one can pretreat with melanin bleach, but this can be time consuming and may result in loss of immunohistochemical reactivity, incomplete melanin removal, or loss of cytologic detail. Kamino and colleagues were the first to report replacement of the counterstain hematoxylin by azure B, which stains melanin green-blue and can be easily contrasted with DAB used in immunohistochemical staining. Thus, the melanocytes appear brown while the melanin granules are green-blue whether in melanocytes, melanophages, pigmented keratinocytes, or free in the dermis ( Fig. 1 B).
Junctional melanocytic proliferations
While S100 is widely believed to be the most sensitive marker for melanocytic lesions, it is also expressed by the Langerhans cells in the epidermis. In addition, it may be easier to interpret nuclear immunohistochemical reactivity in junctional melanocytic proliferations on sun-damaged skin when compared with the often dendritic, cytoplasmic staining of other melanocytic markers that may simulate confluence, an important criterion for diagnosis of melanoma in situ. Although S100 stains the nuclei of melanocytes, it is also a cytoplasmic stain. Therefore the purely nuclear stains, MITF and Sox-10, which do not highlight Langerhans cells, have shown superiority in this context. Sox-10 has the added advantage of also highlighting an occult spindle-cell or desmoplastic melanoma in the underlying dermis, whereas MITF can lack sensitivity in the spindled component.
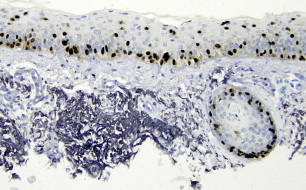
Caution is required because use of purely nuclear melanocytic markers can result in an initial tendency to undercall confluence, as adjacent nuclear staining will not appear to touch because of the intervening cytoplasm ( Fig. 2 ).
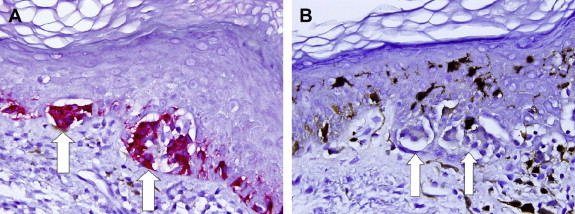
Although uncommon, cells simulating junctional nests on routine sections can react with melanocytic markers and falsely suggest a melanocytic proliferation. These collections of cells have been referred to as pseudonests, and have been reported most commonly with MART-1/Melan-A in the setting of a lichenoid process ( Fig. 3 A). However, a similar pitfall has been reported with MITF and Sox-10. In reality these clusters of cells, when truly not incidental melanocytic nests, are likely an aggregate of cells including keratinocytes and macrophages, potentially in combination with rare melanocytes. The nonspecific staining may result from the lichenoid damage, allowing transfer of melanocyte antigens to adjacent nonmelanocytic cells. Clinical correlation and use of more than one melanocytic marker, including S100, should prevent a misdiagnosis of melanoma in situ ( Fig. 3 B).
Junctional melanocytic proliferations
While S100 is widely believed to be the most sensitive marker for melanocytic lesions, it is also expressed by the Langerhans cells in the epidermis. In addition, it may be easier to interpret nuclear immunohistochemical reactivity in junctional melanocytic proliferations on sun-damaged skin when compared with the often dendritic, cytoplasmic staining of other melanocytic markers that may simulate confluence, an important criterion for diagnosis of melanoma in situ. Although S100 stains the nuclei of melanocytes, it is also a cytoplasmic stain. Therefore the purely nuclear stains, MITF and Sox-10, which do not highlight Langerhans cells, have shown superiority in this context. Sox-10 has the added advantage of also highlighting an occult spindle-cell or desmoplastic melanoma in the underlying dermis, whereas MITF can lack sensitivity in the spindled component.
Caution is required because use of purely nuclear melanocytic markers can result in an initial tendency to undercall confluence, as adjacent nuclear staining will not appear to touch because of the intervening cytoplasm ( Fig. 2 ).
Although uncommon, cells simulating junctional nests on routine sections can react with melanocytic markers and falsely suggest a melanocytic proliferation. These collections of cells have been referred to as pseudonests, and have been reported most commonly with MART-1/Melan-A in the setting of a lichenoid process ( Fig. 3 A). However, a similar pitfall has been reported with MITF and Sox-10. In reality these clusters of cells, when truly not incidental melanocytic nests, are likely an aggregate of cells including keratinocytes and macrophages, potentially in combination with rare melanocytes. The nonspecific staining may result from the lichenoid damage, allowing transfer of melanocyte antigens to adjacent nonmelanocytic cells. Clinical correlation and use of more than one melanocytic marker, including S100, should prevent a misdiagnosis of melanoma in situ ( Fig. 3 B).
Melanoma versus nevus
Of most interest are antibodies that may help in differentiating between benign and malignant melanocytic lesions. However, no single marker or panel of markers proves the diagnosis of melanoma unequivocally. Although trends have been identified, IHC alone cannot predict the biological behavior of a neoplasm.
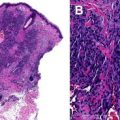
The diminishing gradient of HMB-45 staining from the junction into the dermis suggests maturation in nevi ( Fig. 4 A). This finding is not surprising, considering there is a loss of premelanosomes with maturation. However, as already mentioned, blue and related nevi lack maturation and stain with HMB-45 throughout. Maturation and this orderly gradient is typically lacking in melanoma ( Fig. 4 B). Recently Leleux and colleagues noted the additional caveat of HMB-45 labeling of nevus cells in scar or directly beneath it, creating the impression of loss of gradient, in healed traumatized benign nevi.
MIB-1, an antibody that detects Ki-67, is a marker of cell proliferation. Nuclear expression is identified in cells within the G1, M, G2, and S phases of the cell cycle but not in G0, the resting phase. Increasing expression and thus increasing proliferation is present in malignant melanocytic lesions and is highest in metastatic melanomas. Nevi exhibit reactivity in very few to no dermal melanocytes. If there is reactivity, the proliferating cells tend to be near the dermal-epidermal junction. MIB-1 is not melanocyte specific, and positive melanocytic nuclei must be distinguished from positive admixed, proliferating inflammatory cells. Dual labeling with a cytoplasmic melanocytic marker, such as MART-1, with a contrasting chromogen (AEC vs DAB) allows differentiation ( Fig. 5 ). Proliferating cell nuclear antigen (PCNA) and minichromosome maintenance protein (MCM) have been used similarly to MIB-1 as an indication of proliferation.
Unlike MIB-1, which detects cells in any phase of the active cell cycle, the antibody against phosphohistone H3 (PHH3) only identifies cells in the M phase. Phosphorylation of histone H3 is associated with decondensation of mitotic chromatin in the M phase. Use of this marker allows identification of mitoses at a lower power and improves interobserver and intraobserver agreement over routine microscopy of H&E-stained sections. Negative-staining apoptotic and hyperchromatic nuclei can easily be distinguished from mitotic figures and identification of the mitotic “hot spot” is readily apparent using PHH3 ( Fig. 6 ). Similar to MIB-1, PHH3 is not cell specific, and dual staining with a cytoplasmic melanocytic marker improves reliable identification.
Related posts:
 Cytogenetic and Mutational Analyses of Melanocytic Tumors
Cytogenetic and Mutational Analyses of Melanocytic Tumors
 Fibrous and Fibrohistiocytic Neoplasms
Fibrous and Fibrohistiocytic Neoplasms
 Update on Vascular Neoplasms
Current Understanding of Cutaneous Lymphoma
Direct Immunofluorescence Testing in the Diagnosis of Immunobullous Disease, Collagen Vascular Disease, and Vascular Injury Syndromes
New Directions in Dermatopathology
Update on Vascular Neoplasms
Current Understanding of Cutaneous Lymphoma
Direct Immunofluorescence Testing in the Diagnosis of Immunobullous Disease, Collagen Vascular Disease, and Vascular Injury Syndromes
New Directions in Dermatopathology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


