Analyses of genetic and genomic alterations of melanocytic tumors have not only led to a better understanding of the pathogenesis of melanocytic tumors but also created new opportunities for improvements in diagnostic accuracy in distinguishing nevus from melanoma, and more effective treatments for patients affected by melanoma. Cytogenetic tests have emerged as a promising ancillary method for the workup of diagnostically problematic melanocytic tumors with ambiguous light microscopic features. Mutation analysis not only is important in treatment decision making but also can be used for improved diagnostic accuracy, staging, and prognosis.
- •
Analyses of genetic and genomic alterations of melanocytic tumors have not only led to a better understanding of the pathogenesis of melanocytic tumors but also created new opportunities for improvements in diagnostic accuracy in distinguishing nevus from melanoma, and more effective treatments for patients affected by melanoma.
- •
Fluorescence in situ hybridization is the preferred assay for limited amounts of tissue targeting specific chromosomes commonly altered in melanoma, but not in nevi.
- •
Histopathologic analysis of hematoxylin-eosin–stained tissue sections and correlation with the clinical context remains the gold standard for diagnosing melanoma.
Introduction
Histopathologic analysis of hematoxylin-eosin–stained tissue sections and correlation with the clinical context remains the gold standard for diagnosing melanoma. In most cases, experienced dermatopathologists can make a definitive, reliable, and reproducible distinction between a melanocytic nevus and malignant melanoma. However, this distinction is not always straightforward. A subset of lesions has unusual or atypical histopathologic features. The difficulty in classifying them is reflected in terms such as minimal deviation melanoma , borderline melanocytic tumor , prognostically indeterminate melanocytic tumor , atypical Spitz tumor , atypical spitzoid melanocytic tumor , atypical Spitz tumor of uncertain malignant potential , and atypical blue melanocytic neoplasms .
When pathologists disagree with each other or acknowledge the inability to render a definitive diagnosis based on routine sections, this poses a dilemma for clinicians and patients and leads to concerns and confusion about prognosis and further management. Therefore, pathologists have explored the use of ancillary techniques to improve diagnostic accuracy for problematic melanocytic tumors. Cytogenetic methods have recently gained popularity for distinguishing nevi from melanoma, including fluorescence in situ hybridization (FISH) analysis and comparative genomic hybridization (CGH).
Even when the diagnosis of melanoma has been established, it has become apparent that not all melanomas are the same. Different mutational subtypes have been identified. This subclassification has become relevant in the optimal treatment selection for patients.
Cytogenetic studies
CGH
Technical aspects
CGH is a method to detect copy number changes throughout the genome. Total genomic DNA is isolated from tissue samples (tumor and normal control) and labeled with different fluorochromes. The mixture is then hybridized onto normal metaphase spreads from a healthy donor (classic CGH) or a microarray of mapped clones or genomic DNA (array CGH). Copy number gains or losses are identified based on differences in fluorescence intensities. CGH permits assessment of copy number changes of all chromosomes. However, tumor cell heterogeneity can be a problem. If copy number changes are present only in a minor subpopulation of the total tumor from which DNA is extracted for CGH, they may escape detection. In general, approximately one-third of the tumor should harbor copy number changes for them to be clearly identifiable on CGH.
Clinical utility
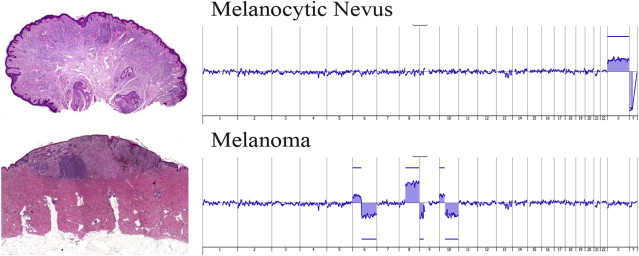
Analysis of melanocytic tumors with CGH revealed that nevi and melanoma differ cytogenetically. Most melanomas show recurrent patterns of chromosomal aberrations, such as losses of chromosomes 6q, 8p, 9p, and 10q, along with copy number gains of 1q, 6p, 7, 8q, 17q, and 20q. In contrast, CGH has shown that most melanocytic nevi lack copy number changes ( Fig. 1 ). Exceptions are rare and include subtypes of Spitz nevus/tumor characterized by gains of 11p or loss of chromosome 3. The lack of significant overlap in the patterns of chromosomal aberrations in melanoma and nevi provides the rationale for using CGH (or FISH; see later discussion) as an ancillary diagnostic tool for diagnostically problematic melanocytic tumors.
CGH has been and is currently most widely used clinically for the workup of diagnostically ambiguous/problematic spitzoid melanocytic proliferations. It can be applied to archival material (formalin-fixed and paraffin-embedded tissue). If a Spitz tumor harbors a copy number gain of 11p, for example, the diagnosis of Spitz nevus can be made with reasonable confidence. However, the detection of multiple copy number changes represents strong evidence in favor of malignant melanoma.
CGH can be applied similarly for ambiguous melanocytic tumors lacking spitzoid features, such as atypical cellular blue nevi or blue nevus–like melanomas. In general, the detection of chromosomal aberrations commonly associated with melanoma, particularly the presence of multiple aberrations, supports a diagnosis of melanoma.
Pitfalls of CGH
CGH-negative malignant melanomas
Although most melanomas show chromosomal aberrations detectable on CGH, not all do. A rare melanoma may be CGH-negative. This finding may be related to test sensitivity or intrinsic biologic reasons. Test sensitivity is an issue when, for example, the quality or amount of extracted DNA is insufficient, or melanocytes with chromosomal aberrations represents only a minor component of the entire tissue used for DNA extraction. Admixed precursor nevomelanocytes and/or stromal/inflammatory cells may dilute the cytogenetically aberrant melanoma, leading to a false-negative CGH result. However, on rare occasions even a uniform malignant tumor cell population may be CGH-negative because of the lack of chromosomal copy number changes.
Benign or indolent melanocytic proliferations with cytogenetic abnormalities
Aberrations of specific chromosomal loci may have much greater significance in diagnosing melanoma. The presence of a single copy number change in just any chromosome per se does not constitute proof of malignancy. A Spitz nevus or tumor, for example, may harbor a gain in 11p or loss of chromosome 3. Other isolated rare copy number changes have also been found in spitzoid melanocytic proliferations lacking overt malignant features and behaving clinically in an indolent fashion. Thus, caution is necessary when confronted with an isolated chromosomal aberration, especially with regard to spitzoid tumors in children. The cytogenetic aberrations of these lesions must be evaluated on an individual basis, taking into account the specific alteration present, the clinical setting, and light microscopic and at times also immunohistochemical findings.
A further limitation of CGH is differentiating heterozygous from homozygous deletions. For example, a loss of a single copy of 9p21 can be seen not only in melanoma but also occasionally in some atypical Spitz tumors with indolent behavior. Alternatively, a homozygous deletion in 9p21 tends to be a much more specific finding for melanoma. This distinction is not always readily apparent on CGH. Hence, the detection of a single copy number aberration including loss of 9p21 should be interpreted with caution and investigated further with FISH.
Cytogenetic studies
CGH
Technical aspects
CGH is a method to detect copy number changes throughout the genome. Total genomic DNA is isolated from tissue samples (tumor and normal control) and labeled with different fluorochromes. The mixture is then hybridized onto normal metaphase spreads from a healthy donor (classic CGH) or a microarray of mapped clones or genomic DNA (array CGH). Copy number gains or losses are identified based on differences in fluorescence intensities. CGH permits assessment of copy number changes of all chromosomes. However, tumor cell heterogeneity can be a problem. If copy number changes are present only in a minor subpopulation of the total tumor from which DNA is extracted for CGH, they may escape detection. In general, approximately one-third of the tumor should harbor copy number changes for them to be clearly identifiable on CGH.
Clinical utility
Analysis of melanocytic tumors with CGH revealed that nevi and melanoma differ cytogenetically. Most melanomas show recurrent patterns of chromosomal aberrations, such as losses of chromosomes 6q, 8p, 9p, and 10q, along with copy number gains of 1q, 6p, 7, 8q, 17q, and 20q. In contrast, CGH has shown that most melanocytic nevi lack copy number changes ( Fig. 1 ). Exceptions are rare and include subtypes of Spitz nevus/tumor characterized by gains of 11p or loss of chromosome 3. The lack of significant overlap in the patterns of chromosomal aberrations in melanoma and nevi provides the rationale for using CGH (or FISH; see later discussion) as an ancillary diagnostic tool for diagnostically problematic melanocytic tumors.
CGH has been and is currently most widely used clinically for the workup of diagnostically ambiguous/problematic spitzoid melanocytic proliferations. It can be applied to archival material (formalin-fixed and paraffin-embedded tissue). If a Spitz tumor harbors a copy number gain of 11p, for example, the diagnosis of Spitz nevus can be made with reasonable confidence. However, the detection of multiple copy number changes represents strong evidence in favor of malignant melanoma.
CGH can be applied similarly for ambiguous melanocytic tumors lacking spitzoid features, such as atypical cellular blue nevi or blue nevus–like melanomas. In general, the detection of chromosomal aberrations commonly associated with melanoma, particularly the presence of multiple aberrations, supports a diagnosis of melanoma.
Pitfalls of CGH
CGH-negative malignant melanomas
Although most melanomas show chromosomal aberrations detectable on CGH, not all do. A rare melanoma may be CGH-negative. This finding may be related to test sensitivity or intrinsic biologic reasons. Test sensitivity is an issue when, for example, the quality or amount of extracted DNA is insufficient, or melanocytes with chromosomal aberrations represents only a minor component of the entire tissue used for DNA extraction. Admixed precursor nevomelanocytes and/or stromal/inflammatory cells may dilute the cytogenetically aberrant melanoma, leading to a false-negative CGH result. However, on rare occasions even a uniform malignant tumor cell population may be CGH-negative because of the lack of chromosomal copy number changes.
Benign or indolent melanocytic proliferations with cytogenetic abnormalities
Aberrations of specific chromosomal loci may have much greater significance in diagnosing melanoma. The presence of a single copy number change in just any chromosome per se does not constitute proof of malignancy. A Spitz nevus or tumor, for example, may harbor a gain in 11p or loss of chromosome 3. Other isolated rare copy number changes have also been found in spitzoid melanocytic proliferations lacking overt malignant features and behaving clinically in an indolent fashion. Thus, caution is necessary when confronted with an isolated chromosomal aberration, especially with regard to spitzoid tumors in children. The cytogenetic aberrations of these lesions must be evaluated on an individual basis, taking into account the specific alteration present, the clinical setting, and light microscopic and at times also immunohistochemical findings.
A further limitation of CGH is differentiating heterozygous from homozygous deletions. For example, a loss of a single copy of 9p21 can be seen not only in melanoma but also occasionally in some atypical Spitz tumors with indolent behavior. Alternatively, a homozygous deletion in 9p21 tends to be a much more specific finding for melanoma. This distinction is not always readily apparent on CGH. Hence, the detection of a single copy number aberration including loss of 9p21 should be interpreted with caution and investigated further with FISH.
FISH analysis
Technical Aspects
In contrast to CGH, FISH targets individual chromosomes or specific regions within a chromosome. Fluorescence-labeled oligonucleotide probes bind to their complementary DNA sequence and label that region, which can then be visualized under a fluorescence microscope ( Fig. 2 ). Two types of probes are currently relevant for the workup of melanocytic tumors. Centromeric probes identify the centromeric region of a specific chromosome and thus help enumerate the number of copies of that chromosome, and allele-specific probes adhere to a specific target sequence such as cyclin D 1 on chromosome 11q or CDKN2A (ie, p16 by its protein name) on 9p21.
Unlike CGH, FISH permits detection of abnormal subpopulations within a heterogeneous tissue mix. Hence, identification of much smaller populations of emerging clones of chromosomally aberrant cells is possible. Visual correlation between a cell nucleus with an abnormal number of chromosomes and cytologic features is possible to verify the identity of an affected cell. Much smaller amounts of tissue are necessary for FISH compared with CGH. For skin biopsies, 1 or 2 unstained 5-μm thin sections of formalin-fixed and paraffin-embedded material usually suffices to perform FISH. The FISH test has 2 major drawbacks. First, it only tests for aberrations in the targeted areas, which is usually limited to 4 chromosomal loci (ie, it does not analyze the entire set of chromosomes as does CGH). Second, depending on the probe set used, the enumeration requires some level of expertise. For example, with the current commercially available melanoma probe set, which targets 3 loci on chromosome 6 and 1 on chromosome 11, tetraploidy can often result in the false impression of copy number gains ( Fig. 3 ). Newer probe sets testing a broader number of chromosomal loci may help diminish this problem.
Several FISH assays are currently available for use in dermatopathology. The so-called melanoma FISH test uses 4 probes, targeting Ras responsive element-binding protein 1 (Vysis LSI RREB1 SpectrumRed), myeloblastosis (Vysis LSI MYB SpectrumGold), cyclin D1 or chromosome 11q13 (Vysis LSI CCND1 SpectrumGreen), and centromeric enumeration probe control for chromosome 6 (Vysis LSI CEP 6 SpectrumAqua), from Abbott Molecular (Des Plaines, IL). The enumeration protocol requires that a total of 30 lesional melanocytes be analyzed per case. A lesion is considered as having a positive FISH result if any of the following criteria are met: (1) gain in 6p25 ( RREB1 ) relative to CEP 6 greater than 55%, (2) gain in 6p25 ( RREB1 ) greater than 29%, (3) loss in 6q23 ( MYB ) relative to CEP 6 greater than 42%, or (4) gain in 11q13 ( CCND1 ) greater than 38%. Additional probes are currently being incorporated into clinical utility, such as those targeting 9p21, which are useful for diagnosing both conventional and spitzoid melanomas, and those targeting 8q24, which are useful for nodular amelanotic and nevoid melanomas.
Other FISH probes of interest for diagnosing melanoma include those targeting chromosome 3 (centromeric probe and bcl2 ) for diagnosing uveal melanoma, and 22q21 ( EWSR1 ) for diagnosing cutaneous clear cell sarcoma (CCS), a soft tissue tumor with melanocytic differentiation, which can be confused with cellular blue nevus, primary nodular or metastatic melanoma (see below).
Utility of the FISH Assay
Distinction of nevus from melanoma
Because conventional nevi tend to lack chromosomal aberrations, but most melanomas harbor copy number changes, a FISH test using probes for chromosomes commonly altered in melanoma should have potential value as an ancillary diagnostic method. Gerami and colleagues documented that such a test could be established and introduced it to the pathology community for diagnosing melanocytic tumors. Using probes targeting loci on 6p, 6q, 6cent, and 11q, they determined cutoff values (see earlier discussion), which permitted a test sensitivity of 85% and specificity of 95% for histopathologically obvious/noncontroversial benign and malignant lesions. Other investigators have reported similar results. Vergier and colleagues’ FISH analysis of 43 nonequivocal melanomas and nevi showed a sensitivity of 85% and specificity of 90%. In a review of 500 cases from a commercial laboratory, 83.8% of melanomas were FISH-positive. Another commercial laboratory analyzed 32 nevi and 31 melanomas using FISH and reported an overall sensitivity of 94% and specificity of 94%. In a recent study from Memorial Sloan-Kettering Cancer Center, test specificity was 98% and sensitivity was 82%.
Several studies confirmed that the FISH test correlates well with consensus diagnoses distinguishing conjunctival nevus from conjunctival melanoma, sclerosing nevus from desmoplastic melanoma, and blue nevus from blue nevus–like melanoma. The test has also been used for diagnosing Spitz nevi. Although Spitz nevi are usually negative, a significant subset of Spitz nevi is tetraploid, which may lead to a false-positive enumeration (see later discussion). For distinguishing Spitz nevus from spitzoid melanoma, the addition of a probe for 9p21 (CDKN2A) has been shown to increase sensitivity and specificity. In fact, a more recently validated probe set targeting 6p25, 11q13, 8q24, and 9p21 has been shown to have an overall improved sensitivity and specificity in distinguishing melanoma from benign nevi, with the probe targeting 9p21 being particularly helpful in identifying spitzoid neoplasms.
Microstaging of primary melanoma
When a melanoma arises in association with a melanocytic nevus, precise assessment of tumor thickness can be problematic. If melanoma cells are distinctly different in appearance from adjacent nevus cells, measurement of Breslow thickness is straightforward. However, thickness may be wrongly measured if the melanoma does not contrast well cytologically with the nevus and the pathologist is uncertain how much of the intradermal melanocytic proliferation is nevus versus invasive melanoma. This possible inaccuracy not only affects the patient’s overall prognosis but also may impact immediate surgical management and staging, such as eligibility for sentinel lymph node biopsy. Using the FISH assay may help in this regard through identifying intradermal melanoma cells with chromosomal gains.
Primary nevus versus nevus-like metastatic melanoma
Metastatic melanoma can occasionally simulate the appearance of a melanocytic nevus. A notorious example is a blue nevus–like melanoma metastasis from primary cutaneous or ocular melanoma. Using the 4-color FISH test, Pouryazdanparast et al documented that chromosomal changes were detected in 9 of 10 blue nevus–like melanoma metastases, but not in a single case of conventional blue nevus. Thus, a positive FISH test can confirm a suspected diagnosis of metastatic blue nevus–like cutaneous melanoma. A different probe set is needed for detecting blue nevus–like uveal melanoma. Because monosomy 3 and amplifications of MYC are common findings in metastasizing uveal melanoma, FISH probes targeting chromosomes 3 and 8 may be useful in diagnosing metastatic blue nevus–like uveal melanoma ( Fig. 4 ). Caution is necessary, however, because cutaneous melanoma and a subtype of Spitz tumor may be associated with loss of chromosome 3 (see later discussion). Furthermore cutaneous melanomas may also have 8q24 gains, particularly amelanotic nodular melanomas in areas of nonchronically sun-damaged skin. Although most metastatic melanomas will show copy number changes detectable on the FISH test, not all do.
Related posts:
 Update on Immunohistochemistry in Melanocytic Lesions
Update on Immunohistochemistry in Melanocytic Lesions
 Fibrous and Fibrohistiocytic Neoplasms
Fibrous and Fibrohistiocytic Neoplasms
 Update on Vascular Neoplasms
Current Understanding of Cutaneous Lymphoma
Direct Immunofluorescence Testing in the Diagnosis of Immunobullous Disease, Collagen Vascular Disease, and Vascular Injury Syndromes
New Directions in Dermatopathology
Update on Vascular Neoplasms
Current Understanding of Cutaneous Lymphoma
Direct Immunofluorescence Testing in the Diagnosis of Immunobullous Disease, Collagen Vascular Disease, and Vascular Injury Syndromes
New Directions in Dermatopathology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


