This article provides an update on vascular neoplasms. New immunohistochemical markers for the diagnosis of vascular neoplasms tumor 1, infantile hemangiomas, myopericytomas, perivascular epithelial cell tumors, acquired elastotic hemangiomas, vascular proliferations in radiated skin, and new histopathologic variants of AIDS-related Kaposi sarcoma are explored.
- •
Wilms tumor 1 (WT1) is a tumor suppressor gene (map locus 11p13).
- •
Myc amplification is found in angiosarcomas secondary to radiation and chronic lymphedema but not in atypical vascular proliferations secondary to radiotherapy.
- •
ERG is also useful in separating angiosarcomas and epithelioid hemangioendotheliomas from their histologic mimics, such as nonendothelial tumors with corded, myxohyaline, and hemorrhagic, highly vascular patterns.
New immunohistochemical markers for the diagnosis of vascular neoplasms
Wilms Tumor 1
Wilms tumor 1( WT1 ) is a tumor suppressor gene (map locus 11p13). The gene product, WT1/Wilms tumor protein, is a transcription factor that contains 4 epidermal growth factor (EGR)–family C2H2-type zinc fingers at 323–347, 353–377, 383–405, and 414–438 and a 57 amino acid, proline-rich region, which recognizes and binds the DNA sequence 5′-CGCCCCCGC-3′. This gene plays an essential role in the normal development of the urogenital system but is also involved in hematopoiesis and angiogenesis. The expression of WT1 is maintained during the differentiation of the various bone marrow stem cells into endothelial cells. WT1 has been detected in acute leukemias, breast carcinomas, melanomas, non–small cell lung cancer, and carcinomas of the genitourinary tract.
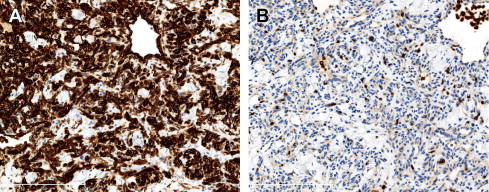
WT1 immunostaining has been used to discriminate between vascular neoplasms and most vascular malformations. A study by Lawley and colleagues showed WT1 expression in infantile hemangiomas (8 of 9), pyogenic granulomas (2 of 2), angiosarcomas (9 of 9), epithelioid hemangioendothelioma (1 of 1), and hobnail hemangiomas (1 of 1). A single case of malignant hemangioendothelioma was negative for WT1. However, vascular malformations (2 port-wine stains, 10 venous malformations, and 8 lymphatic malformations) did not show any positive endothelial staining. More recently Trindade and colleagues, confirmed these results and expanded these findings. They found expression of WT1 in arteriovenous malformations (AVMs), noninvoluting congenital hemangiomas (NICHs) ( Fig. 1 A and B), rapidly involuting congenital hemangiomas (RICHs), tufted angiomas, and spindle cell hemangiomas. They also confirmed the absence of WT1 expression in anomalous vessels in capillary, lymphatic, and venous malformations. All AVMs showed positivity for WT1 in the lesional endothelia; this could be related to the proliferative stage of the AVM, because all their cases were in stage II, with arteriovenous shuntings and clinical enlargement.
Claudins
Claudins are a family of proteins that are components of the tight junctions and are part of the cellular barrier that controls the flow of molecules in the intercellular space between epithelial cells. They have 4 transmembrane domains, with the N -terminus and the C -terminus in the cytoplasm. They are expressed in various endothelia and in some, especially juxtaluminal, glandular and ductal epithelial cells. Claudin-5 is also required in cardiovascular development, and monoallelic loss of a chromosome 22 segment including claudin-5 locus causes velocardiofacial syndrome, including cardiac malformations.
Miettinen and colleagues found that claudin-5 is a sensitive marker for angiosarcoma and hemangioendothelioma but is not very specific, considering its widespread expression in carcinomas. Claudin-5 is significantly expressed in most angiosarcomas, indicating that this cell junction protein is generally conserved in endothelia with malignant transformation. Claudin-5 is very specific for angiosarcomas. Only synovial sarcomas are positive for this antibody. Claudin-5 is useful to differentiate from mimics of angiosarcoma, such as epithelioid sarcoma, and melanoma, which are consistently claudin-5–negative.
Avian V-Ets Erythroblastosis Virus E26 Oncogene Homolog
Avian v-ets erythroblastosis virus E26 oncogene homolog (ERG) is a transcription factor of the erythroblast transformation–specific family. It is expressed in the nuclei of endothelial cells and in normal lymphatics. It is also expressed in subsets of prostatic carcinoma, acute myeloid leukemia, and Ewing sarcoma.
ERG stain is a highly specific endothelial marker for vascular neoplasms. It can be useful in differentiating hemangiomas, which have a dual cell population (ERG-positive endothelial cells and ERG-negative nonendothelial components, especially pericytes) from angiosarcomas, which generally have only ERG-positive endothelial components.
ERG is also expressed in malignant vascular endothelial neoplasms (hemangioendotheliomas, angiosarcomas, and Kaposi sarcomas). The staining is usually seen in most tumor cells, indicating that the expression of the ERG transcription factor in endothelial cells and angiosarcomas is an all-or-none phenomenon. ERG is also useful in separating angiosarcomas and epithelioid hemangioendotheliomas from their histologic mimics, such as nonendothelial tumors with corded, myxohyaline, and hemorrhagic, highly vascular patterns.
ERG is more specific than other endothelial markers, such as CD31, the current gold standard in the definition of angiosarcoma. ERG immunoreactivity is highly endothelium-restricted and straightforward to interpret, whereas interpretation of CD31 can be problematic, because it also stains histiocytes and plasma cells, which can lead to an overdiagnosis of angiosarcoma. CD31 also stains platelets.
c- Myc
c- Myc is a regulator gene that codes for a transcription factor. A mutated version of Myc is found in many cancers, which causes Myc to be constitutively (persistently) expressed. This function leads to the unregulated expression of many genes, some of which are involved in cell proliferation and results in the formation of cancer.
A common translocation involving Myc is t(8;14). This translocation is found in some malignant neoplasms, including secondary but not primary angiosarcomas. This is the most frequent recurrent alteration on chromosome 8q24.21 (50%), followed by 10p12.33 (33%) and 5q35.3 (11%).
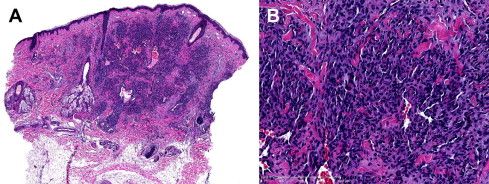
Myc amplification is found in angiosarcomas secondary to radiation and chronic lymphedema ( Fig. 2 A–C), but not in atypical vascular proliferations secondary to radiotherapy.
Infantile hemangiomas
Infantile hemangioma (IH) is the most common benign vascular proliferation, and traditionally has been considered a neoplasm. This classification may be true for a minority of these proliferations, but most IHs are better considered as hyperplasias. Classical IHs, after an initial proliferative phase, undergo complete regression, through a process of fibrosis, even in the absence of therapy. The histopathologic composition of IHs varies with the age of the lesion. Early hemangiomas are highly cellular and are characterized by plump endothelial cells aligned to vascular spaces with small inconspicuous lumina. As the lesions mature, blood flow increases, endothelium flattens, and the lumina of the vessels enlarge and become more obvious. During this interval, the vessels convey a “cavernous” appearance that can be misinterpreted as a venous malformation. Regression is portrayed as progressive interstitial fibrosis and adipose metaplasia, a process without known stimulus.
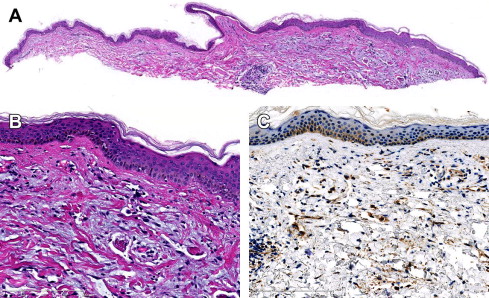
The other 2 types of IH include NICH and RICH. NICH is a rare true vascular tumor that is fully formed at birth, grows proportionally with the patient or expands slightly over time, and does not regress. RICH is also fully formed at birth but completely regresses within the first 6 months to 1 year of life. NICH is characterized by the presence of lobular collections of small, thin-walled vessels with large, often stellate, central lumina, separated by variable amounts of fibrous tissue richly supplied with normal and abnormal veins and arteries ( Fig. 3 ).
These vascular proliferations differ from IH in their growth patterns and lack of immunoreactivity for the glucose transporter-1 protein (GLUT1), which is a sensitive and specific marker for IH (see Fig. 1 B). This protein is not detectable in the blood vessels of normal skin or in most other types of vascular tumors but is highly expressed in endothelia at sites of blood-tissue barriers, which include the brain and placenta.
Infantile hemangiomas
Infantile hemangioma (IH) is the most common benign vascular proliferation, and traditionally has been considered a neoplasm. This classification may be true for a minority of these proliferations, but most IHs are better considered as hyperplasias. Classical IHs, after an initial proliferative phase, undergo complete regression, through a process of fibrosis, even in the absence of therapy. The histopathologic composition of IHs varies with the age of the lesion. Early hemangiomas are highly cellular and are characterized by plump endothelial cells aligned to vascular spaces with small inconspicuous lumina. As the lesions mature, blood flow increases, endothelium flattens, and the lumina of the vessels enlarge and become more obvious. During this interval, the vessels convey a “cavernous” appearance that can be misinterpreted as a venous malformation. Regression is portrayed as progressive interstitial fibrosis and adipose metaplasia, a process without known stimulus.
The other 2 types of IH include NICH and RICH. NICH is a rare true vascular tumor that is fully formed at birth, grows proportionally with the patient or expands slightly over time, and does not regress. RICH is also fully formed at birth but completely regresses within the first 6 months to 1 year of life. NICH is characterized by the presence of lobular collections of small, thin-walled vessels with large, often stellate, central lumina, separated by variable amounts of fibrous tissue richly supplied with normal and abnormal veins and arteries ( Fig. 3 ).
These vascular proliferations differ from IH in their growth patterns and lack of immunoreactivity for the glucose transporter-1 protein (GLUT1), which is a sensitive and specific marker for IH (see Fig. 1 B). This protein is not detectable in the blood vessels of normal skin or in most other types of vascular tumors but is highly expressed in endothelia at sites of blood-tissue barriers, which include the brain and placenta.
Related posts:
 Cytogenetic and Mutational Analyses of Melanocytic Tumors
Cytogenetic and Mutational Analyses of Melanocytic Tumors
 Dermatology Clinics
Fibrous and Fibrohistiocytic Neoplasms
Current Understanding of Cutaneous Lymphoma
Direct Immunofluorescence Testing in the Diagnosis of Immunobullous Disease, Collagen Vascular Disease, and Vascular Injury Syndromes
New Directions in Dermatopathology
Dermatology Clinics
Fibrous and Fibrohistiocytic Neoplasms
Current Understanding of Cutaneous Lymphoma
Direct Immunofluorescence Testing in the Diagnosis of Immunobullous Disease, Collagen Vascular Disease, and Vascular Injury Syndromes
New Directions in Dermatopathology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


