Umbilicoplasty
Sergey Y. Turin
Chad A. Purnell
Gregory A. Dumanian
DEFINITION
Reconstruction of the umbilicus is an essential part of restoring the natural aesthetic of the abdomen.
It is the focal point of the anterior abdominal wall, helps define the middle abdominal sulcus and if absent or malformed, will draw attention to the abdomen.1
We present two simple techniques for creation of a neoumbilicus.
One is to be used for patients with vertical midline incisions.
The other is for patients undergoing abdominoplasty when the umbilical stalk cannot be maintained.
Umbilicoplasty for a scarred umbilicus after a standard abdominoplasty will also be discussed.
ANATOMY
The umbilicus is generally described as a depressed circular indentation approximately 1.5 to 2 cm in diameter positioned in the midline of the abdomen at the level of the superior iliac crests2 (FIG 1A).
The vertical position has also been variably described as 30% to 47% of the way up between the symphysis pubis and the xiphoid.3,4
The aesthetic ideal of the female umbilicus has been described as T or vertical in shape with a superior hood or shelf.1 Protrusion, transverse orientation, or excessive size are rated as less attractive. There is a linear depression running from the xiphoid to the umbilicus, and this compares to the smooth contour of skin without a depression from the umbilicus to the symphysis pubis. Surrounding the umbilicus is a zone of decreased fat approximately 3 cm in diameter total, and this fat thickens to its maximum dimension for the ventral abdomen over the anterior rectus fascia.
PATIENT HISTORY AND PHYSICAL FINDINGS
Past surgical history, including prior transection of the umbilical stalk at the time of an umbilical hernia repair, must be obtained. Prior laparoscopy umbilical portal sites can be the cause of incisional hernias and scar formation around the umbilicus.
A reversed sit-up maneuver should be done for evaluation of rectus diastasis.
Significant abdominal hirsutism should be appreciated preoperatively and is a relative contraindication to umbilicoplasty, as hair-bearing skin is placed deep against the abdominal wall and could create an iatrogenic pilonidal cyst.
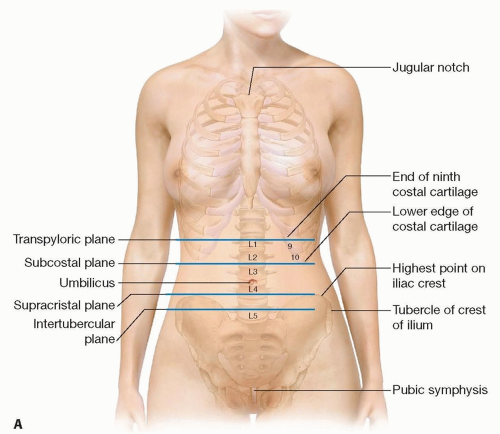 FIG 1 • A. Location of umbilicus. |
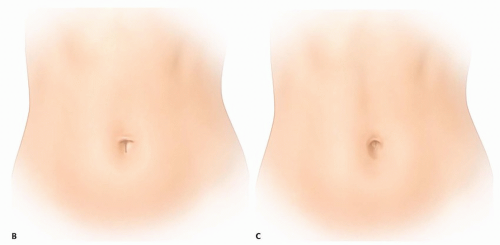 FIG 1 (Continued) • B. T-shaped umbilicus. C. Aesthetic abdominal contour with supraumbilical depression. |
SURGICAL MANAGEMENT
Preoperative Planning
The decision-making process for umbilicoplasty begins in the operating room after repair of the rectus muscles in the midline. The critical issue is whether or not the umbilical stalk remains vascularized and attached to the abdominal wall. For midline laparotomies, there is typically skin excess, and we find it easier to discard a marginal umbilical stalk and simply reconstruct it with pumpkin-teeth flaps.
Patients undergoing an abdominoplasty where the stalk will not remain viable will need to be counseled that the reconstructed umbilicus with local flaps is not as aesthetic as the umbilical stalk that they currently have.
Positioning
The patient is positioned in the usual supine position. The entire abdomen from xiphoid to pubis should be prepped to allow accurate determination of the midline and landmarks for appropriate umbilicus positioning.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree