Festoons represent a combination of fluid accumulation and soft tissue laxity in the superolateral cheek. They remain a difficult entity to treat. The ideal treatment for festoons would possess minimal invasiveness and recovery time, and predictably improve the condition. No nonsurgical treatment currently meets these criteria, and surgical treatments have significant limitations. Fortunately, a variety of treatment options exist that can benefit each patient and be tailored to their specific needs. Knowledge of the underlying anatomy, clinical characteristics, and clinical evaluation will better equip the treating physician to manage festoons.
Key points
- •
Festoons are also referred to as malar mounds and malar edema. No clear nomenclature exists to describe these lesions.
- •
Nonsurgical options for treating festoons include fillers, laser and trichloroacetic peels, radiofrequency thermoplasty and microneedling, and sclerosing therapies such as deoxycholic acid, tetracycline, and doxycycline injections.
- •
Surgical options include direct excision, skin muscle flap, extended blepharoplasty and midface lift.
- •
Although a variety of treatments options exist, festoons remain frustrating to the patient and challenging for the surgeon.
Introduction
The lack of clear nomenclature to describe the deficit in the superolateral cheek beneath the eyelid/cheek junction termed a “festoon” parallels our lack of understanding of this condition, yet the phenotype of this crescentic triangular sagging, with or without fluid accumulation, is as unmistakable as it is frustrating to both the patient and the surgeon. This article aims to present our current understanding and treatment of the conditions widely known as “festoons.”
Festoons background, etiology, and anatomy
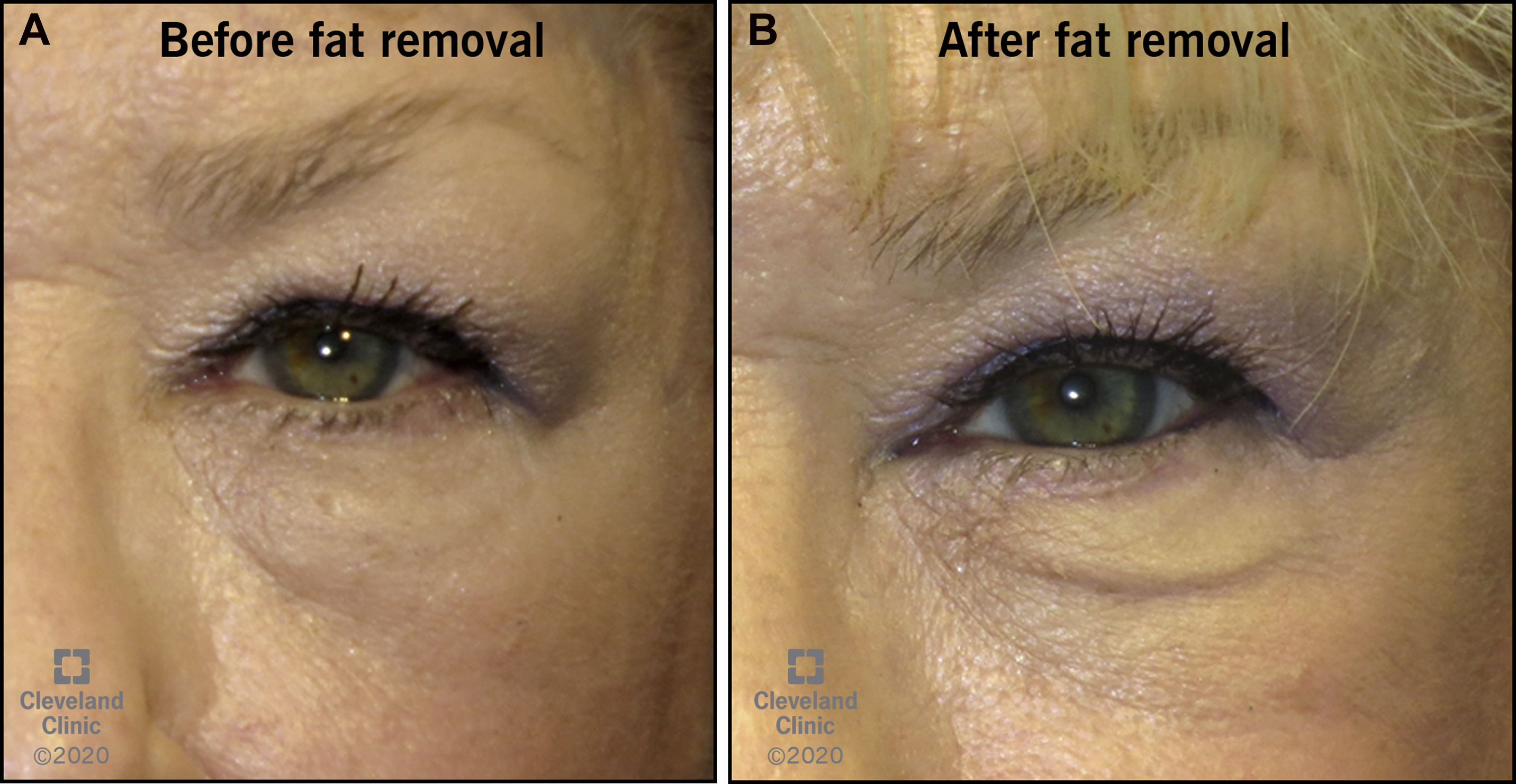
The clinicopathology of festoons and malar mounds is not well understood. These lesions may appear with age as tissues gradually descend in a redundant fashion over the malar eminence; however, they can also occur early in life. Some patients may not notice a festoon until it is pointed out to them, or in unfortunate cases, only after blepharoplasty has hollowed the lower eyelids to unmask it ( Fig. 1 ).
A combination of tissue laxity (skin and orbicularis oculi), a weakened orbital retaining ligament, and weakening of the firm attachment of the inferiorly located zygomaticocutaneous ligament (ZCL) can lead to inferior displacement of the skin and orbicularis, forming a bulge over the prezygomatic region. , Fluid buildup in this region can accompany the redundant anterior tissues.
Terminology
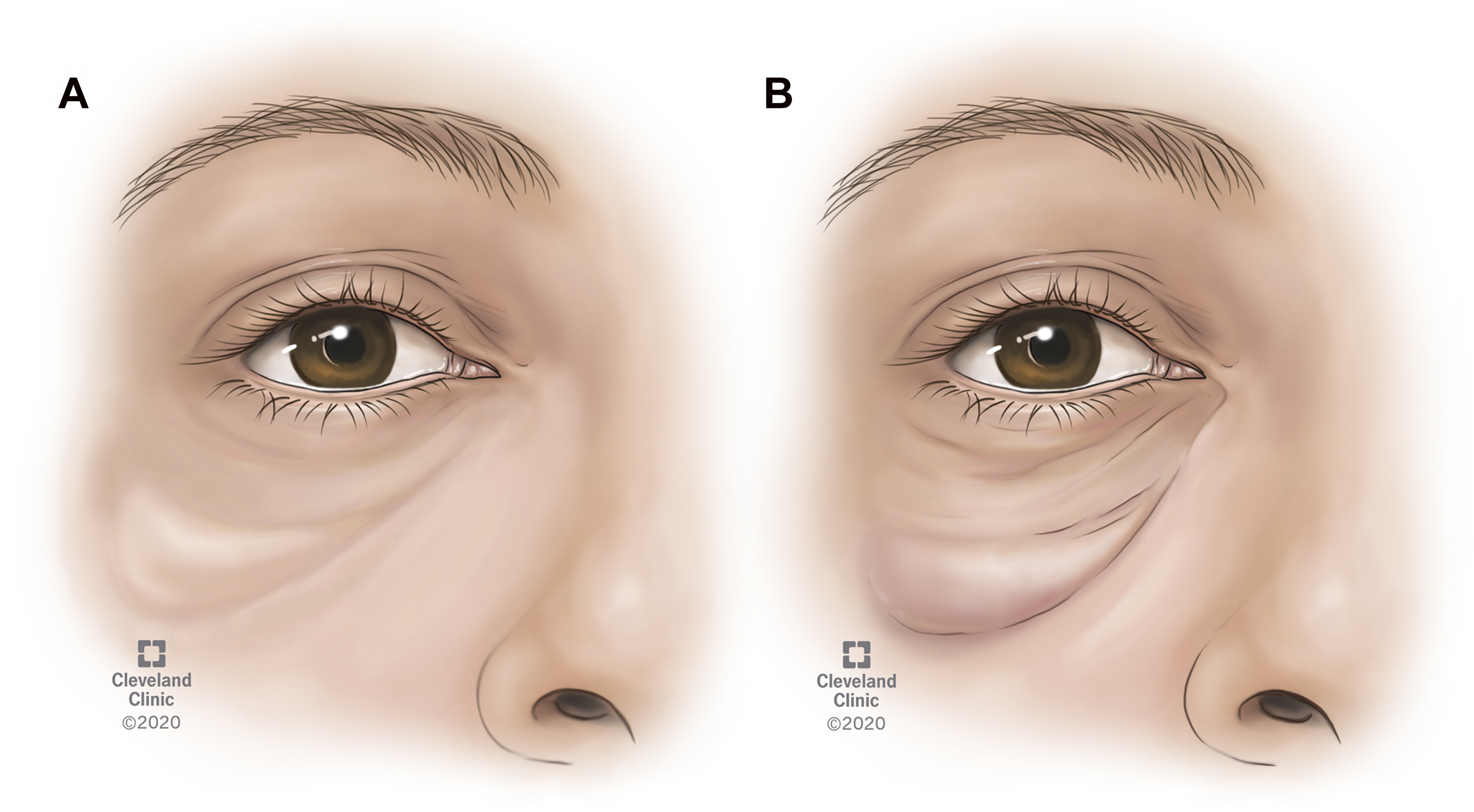
Several terms are used to describe festoons, including malar mounds, malar edema, saddle bags, fluid bags, palpebral bags, and lower eyelid bags. Kpodzo and colleagues suggest using 3 distinct terms: malar edema, malar mound, and festoons. Malar edema refers to fluid over the malar eminence. Malar mound refers to soft tissue prominence, usually orbicularis muscle or fat, over the malar eminence. Finally, festoons refer to the “cascading hammocks of lax skin and orbicularis muscle that hang between the medial and lateral canthi.” Although these 3 terms may represent distinct entities, they may represent points on the spectrum of the same pathophysiologic condition. In this article the term “festoon” is used to encompass the entire spectrum of fluid-associated mounds over the malar eminence ( Fig. 2 ).
Anatomy
To understand festoons, a brief description of the anatomy is instructive. The prezygomatic space or festoon space is marked superiorly and inferiorly at the lid–cheek junction and the midcheek, respectively. The upper border is marked by the orbitomalar ligament (OML), the lower border by the ZCL. Malar bags/festoons are consistently found approximately 2.5 to 3.0 cm below the lateral canthus.
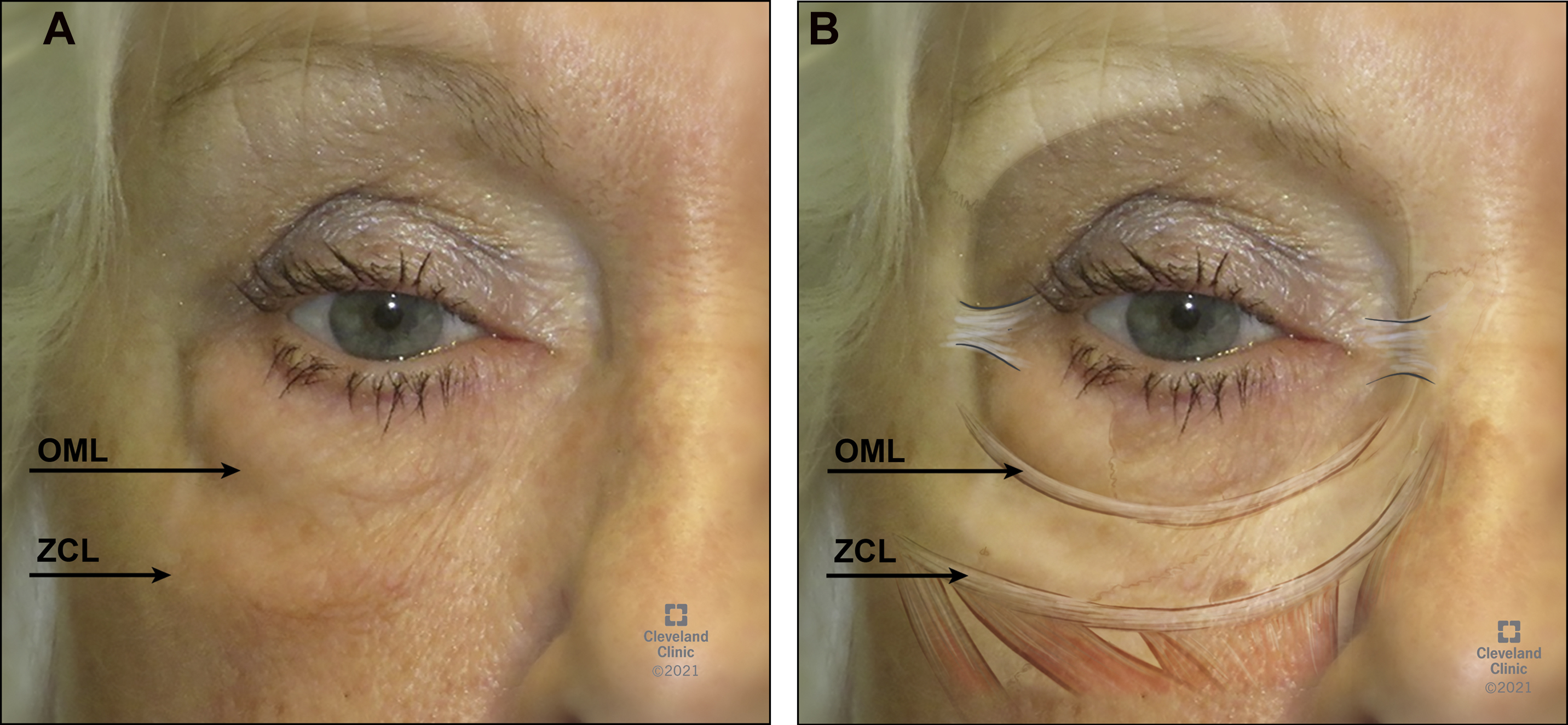
The upper border of a festoon is at the lateral lid–cheek junction. The OML, described by Kikkawa and colleagues, coincides with the boundary. The OML is a soft tissue structure which originates at the inferior orbital rim/arcus marginalis and courses through the orbicularis oculi muscle, and inserts into the dermis, at the level of the lid–lower eyelid cheek transition. The insertion corresponds with both the lid–cheek junction laterally and the and nasojugal groove medially. The OML has connective tissue components (collagen and elastin) that undergo involutional change with age (Kikkawa and colleagues ) and elongate, which allows tissue ptosis and contribute to the appearance of festoons. The OML is also important in the appearance of lower eyelid orbital fat prolapse. The OML acts as the inferior boundary of orbital fat prolapse and thus can enhance the appearance of eyelid bags. , Orbital fat prolapse is a commonly encountered age-related change that occurs superior to the OML. This characteristic distinguishes it from festoons, which are located below the OML ( Fig. 3 ).
Medially, the upper and lower boundaries of the festoon converge, approximately at the mid-pupil line. In this area, there is a convergence of the palpebromalar groove superiorly, the tear trough medially, and the midcheek groove or nasojugal fold inferiorly, giving a Y-shaped appearance.
The malar septum originates at the inferior orbital rim, descends inferiorly through the suborbicularis oculi fat (SOOF), penetrates the orbicularis oculi before inserting into the mid-cheek dermis. It is thought that the interdigitation of the malar septum with the fibrous septa of the SOOF fat creates an impermeable barrier from the orbital rim to the cheek skin. The function of the malar septum is postulated to partition the eye from the lower face.
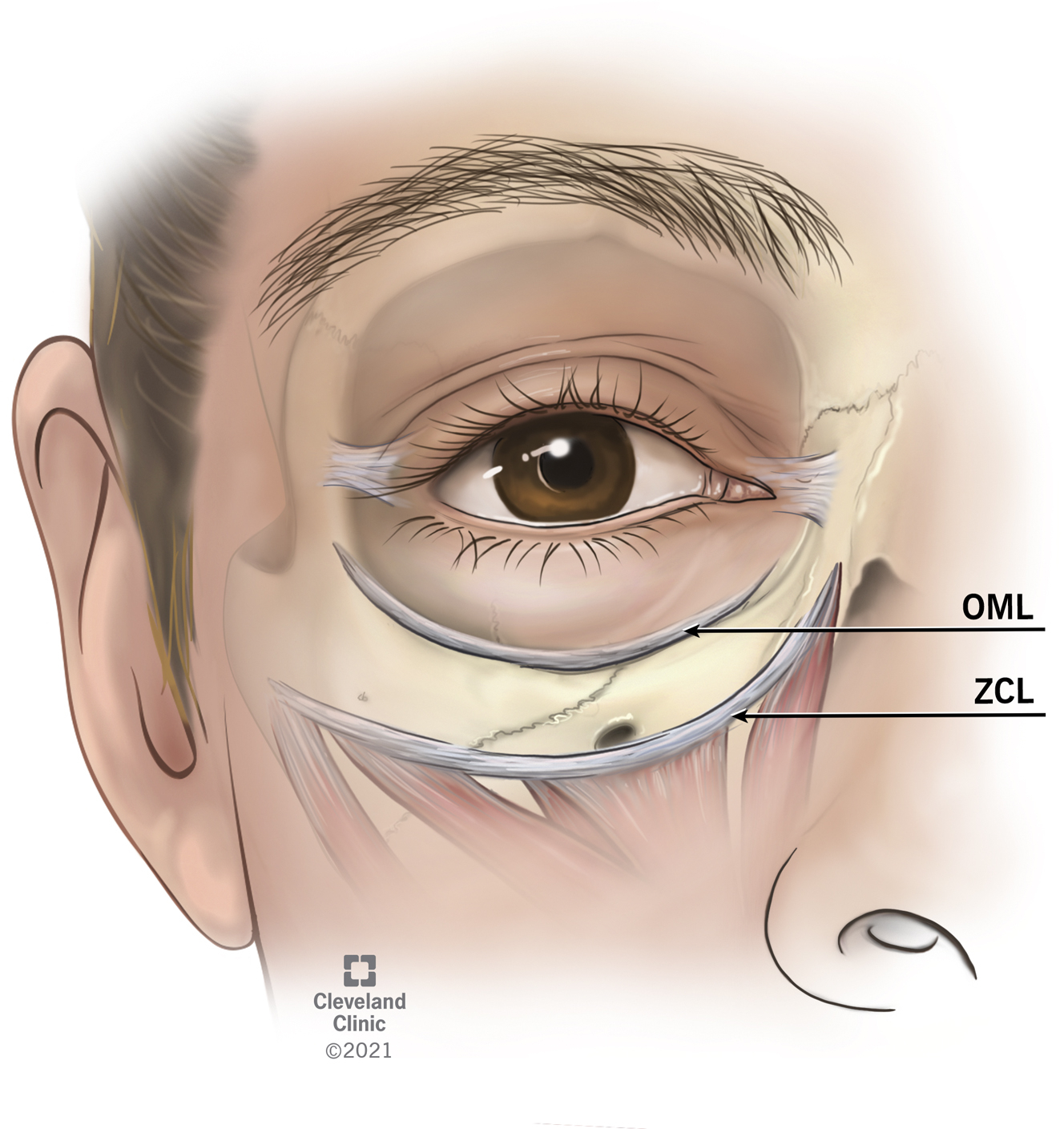
The inferior border of the festoon is at the ZCL. Mendelson and colleagues described the inferior border of the prezygomatic space as the ZCL. The zygomatic ligaments are stronger than the OML. The zygomatic ligaments originate from the periosteum of the zygoma near the origins of the zygomaticus major, zygomaticus minor, and levator labii superioris ( Fig. 4 ). The ZCL extends anteriorly into the overlying soft tissue and dermis, forming the midcheek furrow.
Characteristics of Festoons
Festoons act as a fluid sponge. Patients with malar mounds tend to be predisposed to prolonged postoperative swelling, suggesting a lymphatic origin for festoons. Shoukath and colleagues evaluated the lymphatic drainage of the lower eyelid region. The lymphatic drainage of the eyelid is composed of both a superficial and deep lymphatic system. Relevant to festoons, the deep lymphatic vessels travel within the roof of the prezygomatic space traveling deep to the preseptal orbicularis oculi, travel within the SOOF space, and then eventually drain into the preauricular lymph nodes and submandibular lymph nodes.
Periocular edema can present both as generalized eyelid puffiness as well as festoons, and both can be caused or aggravated by a variety of inflammatory conditions, such as postoperative edema and systemic malignancies, such as angiosarcoma or lymphoma. , Specific systemic inflammatory causes of facial edema and/or festoons include acne rosacea, acne vulgaris, systemic lupus erythematosus, sarcoidosis, allergic dermatitis, dermatomyositis, and angioedema. Periocular topical medications causing blepharitis and conjunctivitis can also produce eyelid edema and festoons, including drops such as apraclonidine, brimonidine, dorzolamide, and pilocarpine, and ointments such as bacitracin and erythromycin. Allergies may include drug-related blepharoconjunctivitis, as well as vernal keratoconjunctivitis and contact dermatitis. Some additional causes of contact dermatitis that might produce eyelid edema and festoons include cosmetics, occupational allergens, hair dyes, nail polishes, and sunscreens.
The most common inflammatory condition associated with festoons is ocular rosacea. Ocular rosacea is a chronic inflammation of the periocular skin associated with erythematous and thickened skin and telangiectasias, papules, and pustules. This condition may lead to conjunctival chemosis and hyperemia, erythema, and thickening of the eyelid margin from meibomitis and blepharitis, as well as periocular skin telangiectasias, erythema, and eyelid swelling. Chronic eyelid lymphedema and festoons can result from chronic rosacea. , , In severe cases, rosacea can be associated with lymphedema of the eyelids, known as Morbihan disease. Chronic inflammation from acne rosacea may cause fibrosis, loss or destruction of elastin around lymphatic vessels, and cause the obstruction of lymphatic vessels leading to lymphedema that presents in the periocular region. ,
Eyelid and cheek tissue laxity contribute to the appearance of festoons. In 1 study, the appearance of festoons and malar bags were compared in participants between upright position and supine positioning. Tear trough, cheek volume, steatoblepharon, malar bags, and nasolabial folds were all significantly decreased in supine positioning. Malar bags and festoons were less prominent with supine positioning in 84% of cases.
Festoons can occur without tissue laxity as well. Some individuals present with festoons at an early age, before significant aging changes appear in the lower eyelid and cheek regions. Occasionally, festoons can occur in early childhood or at birth and are known as congenital festoons. It is unclear whether festoons that present earlier in life possess a different pathophysiology from festoons that occur later in life. Acquired festoons are improved with forceful closure of the eyes, improve with laterally pulling of the lower eyelid upwards and laterally, and worsen with botulinum toxin. In patients with congenital festoons, forceful closure and lateral pulling improve but do not resolve the festoon, and the festoon does not change with botulinum toxin injections.
Festoons can worsen in a variety of clinical settings. Malar mounds or festoons may be prominent in patients with thyroid disorders and those with allergies, as well as postoperatively with infraorbital incisions. Other causes of malar bags include patients with systemic disease such as chronic renal disease, allergy, or hepatic cirrhosis. Postoperative edema is thought to be a combination of postoperative inflammation and lymphatic dysfunction. Eyelid lymphedema has also been noted to occur after neck dissection and radiotherapy for metastatic squamous cell carcinoma to cervical lymph nodes. It is thought that submandibular and deep cervical lymph node removal can lead to chronic lymphedema.
Case reports have noted festoon formation after botulinum toxin injections. In 1 case study, botulinum toxin was injected into the lateral canthus and infraorbital region. One theory for the formation of the festoon was weakening of the orbicularis oculi pumping mechanism, leading to localized lymphedema. Asaadi refer to this as a “positive botox test” in acquired festoons, because a weakening and laxity of the orbicularis oculi can contribute to the formation of festoons, with worsening of festoons with botulinum toxin noted in acquired festoons, although not seen with congenital festoons.
Hyaluronic acid gel (HAG) fillers can worsen or possibly even cause festoons. Owing to the hydrophilic nature and isovolemic degradation of HAG fillers, these products when injected in the periocular region can worsen or potentially even cause festoons. Fillers injected into the periorbital hollows may result in malar edema in as many as 15% of patients. Improvement can occur after injection of hyaluronidase, but some festoons persist even after multiple hyaluronidase injections. HAG filler treatment in the tear trough and midface area is an increasing and troublesome cause, as well as an aggravating factor, in patients presenting with festoons.
Evaluation
Relevant Medical History
Before considering treatment options, it is important to evaluate for treatable or modifiable contributing factors to eyelid edema. A significant number of medications can cause eyelid edema, some including acetaminophen, aspirin, nonsteroidal anti-inflammatory drugs, hormonal supplements, and prednisone, among many other medications. In addition to oral medications, a variety of topical ophthalmic eyedrops and ointments can cause either blepharoconjunctivitis or medication allergy that can contribute to eyelid edema. In suspected medications, if possible the medication should be held for at least 2 weeks to evaluate for causation.
Medical conditions that can contribute to eyelid edema include ocular rosacea, thyroid eye disease, floppy eyelid syndrome, obstructive sleep apnea, and blepharochalasis. Conditions leading to systemic edema such as cardiac, renal hepatic disease, low protein states, lymphatic obstruction, and hypothyroidism can contribute to eyelid edema. Allergic conditions can also worsen festoons, whether environmental, drug related, or other causes of hypersensitivity reactions. Signs of allergy include itching, vertical eyelid rhytids, eyelid erythema, and thickening.
Clinical Evaluation
It is important to differentiate between causes of lower eyelid bags. Festoons should be differentiated from lower eyelid fat prolapse, or steatoblepharon. Lower eyelid fat prolapse is located above the location of a festoon. Fat prolapse presents as fullness in the lower eyelid, above the OML. Although orbital fat in a young individual is located with the orbital space above the inferior orbital rim, with aging changes the fat can drape over and below the inferior orbital rim. Festoons present as a triangular shape below the OML and inferior orbital rim, in the area of the cheek. A festoon will always be located inferior to prolapsed orbital fat.
Once correctly identified, the festoon can then be further evaluated. The pinch test is 1 method of evaluating festoons. The clinician pinches the festoon skin at various sites to assess for the degree of orbicularis oculi bulk contributing to the festoon. This test can be used to differentiate between a predominantly fluid-filled structure from a predominantly soft tissue one.
An additional test, the squinch test, evaluates the orbicularis oculi muscle as the patient squeezes their eyelids tightly closed. This maneuver demonstrates the maximum contraction of the orbicularis oculi and highlights the degree of muscle involvement in the appearance of the festoon. In orbicularis laxity, the squinch test should significantly improve the appearance of festoons. If orbital fat is a contributing factor then the fat portion will not be effaced by the maneuver, but rather dislocated.
Because some of the surgical options for festoon management incorporate lower eyelid tightening, lower eyelid laxity should be evaluated using the snapback test and/or the eyelid distraction test.
Festoons management: nonsurgical
A variety of nonsurgical treatments have been attempted to improve festoons.
Although HAG fillers can worsen festoons, they can be used carefully to try to conceal them The filler material can be injected into the surrounding areas of volume loss. High viscosity filler material may also cause a “posterior girdle” effect to improve the appearance of festoons. Overcorrection can lead to worsening distension of weak ligaments in the area (such as the OML) and even cause postinjection edema that worsens festoons, particularly if there are already disrupted lymphatics. The pros and cons of this approach must be carefully weighed with the patient because some filler-related worsening of festoons may not be reversible with hyaluronidase.
Hyaluronidase has been used for non–filler-related festoons. Some patients with idiopathic edema and no known history of filler use had some improvement in their festoons with hyaluronidase injection. However, in our practice, this effect seems to be temporary at best. Oral diuretics are also another option, but again we have not noticed predictable improvement in our patients who have tried this option. Spironolactone (Aldactone) in doses of 25 to 100 mg/d are generally used.
Laser treatment with CO 2 and Er:YAG ablative lasers have been described for the treatment of malar bags. Because there is no repositioning of soft tissue, the treatment is best served for mild festoons or with mild excess skin laxity. Risks include pigmentary changes, scarring, ectropion, and eyelid retraction.
Radiofrequency microneedling has been attempted for festoons. , Jeon and Geronemus published a report of 2 patients who had improvement of festoons using microneedle radiofrequency technology. The procedure benefits from being noninvasive can be repeated. Bipolar radiofrequency microneedling works by delivering thermal injury to the dermis and fat and is thought to improve rhytids by increasing collagen and elastic fibers. Other nonsurgical treatment options include radiofrequency thermoplasty and trichloroacetic acid or other chemical peels.
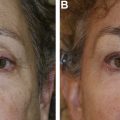
Tetracycline injections have been used for the reduction of festoons ( Fig. 5 ). Tetracycline has been used in other areas of the body for its sclerosing properties. The exact mechanism of action is not known, although it is thought that the ability of tetracycline to inhibit matrix metalloproteinases and growth factor–like activity to stimulate fibroblast proliferation contribute to the ability of sclerodesis of the festoon space. Complications including ischemia, necrosis, persistent postinjection pain, and nerve palsies were not seen. , The authors inject tetracycline 2%, 0.2 to 0.5 mL per lesion ( Fig. 6 ). It may take weeks to see the effect, and we have injected some festoons more than once, at least 90 days apart. Festoons that are not related to hyaluronic acid filler injection seem to respond best to the injection.

Related posts:
 Blepharoptosis Repair: External Versus Posterior Approach Surgery: Why I Select One over the Other
Blepharoptosis Repair: External Versus Posterior Approach Surgery: Why I Select One over the Other
 Transconjunctival Lower Lid Blepharoplasty with and Without Fat Preservation and Skin Resurfacing
Transconjunctival Lower Lid Blepharoplasty with and Without Fat Preservation and Skin Resurfacing
 The Treatment of Post-blepharoplasty Lower Eyelid Retraction
The Treatment of Post-blepharoplasty Lower Eyelid Retraction
 My Evolution with Endoscopic Brow-Lift Surgery
My Evolution with Endoscopic Brow-Lift Surgery
 Transcutaneous Blepharoplasty with Volume Preservation
Transcutaneous Blepharoplasty with Volume Preservation
 Periorbital Fat Grafting
Periorbital Fat Grafting
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


