Transconjunctival lower lid blepharoplasty is a safe and effective procedure with a low complication rate. Success with this procedure depends on proper patient analysis and selection. The lower lid periorbital fat can be resected, or preserved, and draped over the orbital rim or used as free fat grafts, depending on the clinical presentation. The lower lid skin can be resurfaced with a peel, with a laser, or by skin pinch depending on surgeon preference.
Key points
- •
Transconjunctival lower lid blepharoplasty is a safe and effective procedure with a low complication rate.
- •
Success with this procedure depends on proper patient analysis and selection.
- •
The lower lid periorbital fat can be resected or preserved and draped or grafted over the orbital rim, depending on the clinical presentation.
- •
The lower lid skin can be resurfaced with a peel, with a laser, or by skin pinch depending on surgeon preference.
History and development of the transconjunctival approach
The transconjunctival blepharoplasty, first introduced in the 1920s, gained widespread popularity in the 1990s with the work of Zarem and Resnick. The transconjunctival approach was popularized as a technique to address periorbital aging while minimizing complications related to the traditional transcutaneous lower blepharoplasty. The traditional lower blepharoplasty, performed through an external approach using a skin-muscle flap technique, was criticized heavily for its association with lower lid malposition and ectropion. In hindsight, this association was largely due to surgical technique and a failure to perform concomitant canthal support procedures.
Continued advances in blepharoplasty techniques and an improved understanding of aging have increased the safety and efficacy of lower blepharoplasty overall. Contemporary blepharoplasty emphasizes lateral canthal support and re-creation of a youthful transition of the lower lid-cheek junction. Generally, the paradigm has shifted toward tissue preservation and augmentation. Even so, when compared with a transcutaneous approach to lower blepharoplasty, the transconjunctival approach offers advantages, including less visible scarring and less downtime. When combined with ancillary techniques, such as skin resurfacing, skin pinch excision, and proper fat management, the transconjunctival approach addresses many of the signs of periorbital aging once thought to only be addressed with a transcutaneous approach. ,
Anatomy of the lower lid
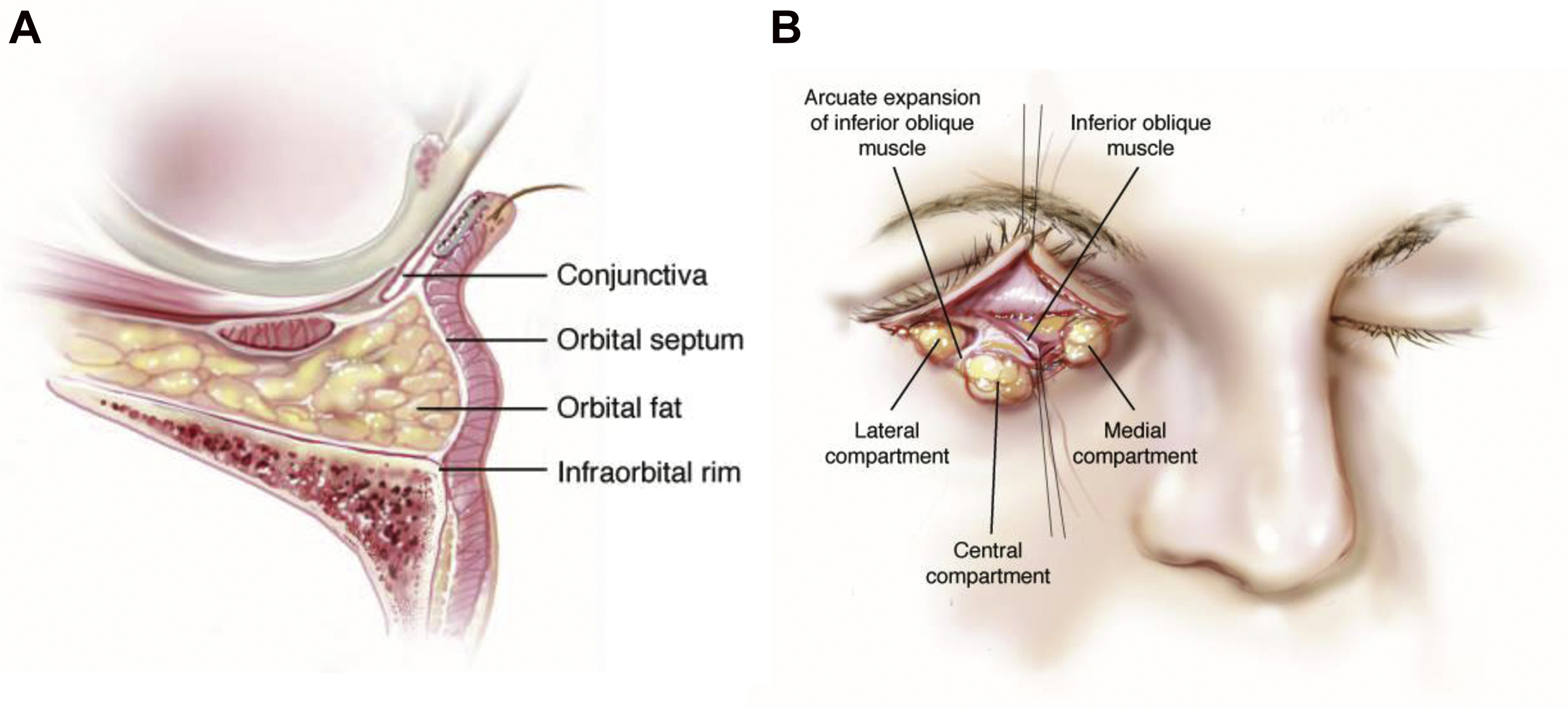
An understanding and ability to visualize lower lid anatomy, inside out and outside in, are paramount to safely performing blepharoplasty and effectively smoothing the lid-cheek junction ( Fig. 1 ).
The lower lid can be divided into 3 lamellae, or layers, each of which has its own functional importance and surgical correlate: the anterior, middle, and posterior.
The anterior lamella, or outermost layer, consists of the thin lower eyelid skin and the concentric orbicularis oculi muscle.
The eyelid skin is the thinnest in the body, at about 0.7 mm thick. There is a delicate surgical plane between the lower eyelid skin and orbicularis oculi muscle.
The orbicularis oculi can be divided into 3 functional portions: pretarsal (overlying the tarsus), preseptal (overlying the septum), and preorbital (overlying the orbital bone). The pretarsal portion of the muscle helps in maintaining lower lid tone and involuntary blink. As such, it is preserved regardless of the type of procedure performed in order to minimize the risks of lid malposition and ectropion. The transition of the preseptal to preorbital portion of the orbicularis oculi is the transition from lid to cheek, defined by the orbicularis retaining ligament (ORL). A further division is made between the medial orbicularis and centrolateral portion of the muscle. This division is defined by innervation and thus function. The inner aspect is driven principally by the buccal branch of the facial nerve and is responsible for involuntary blinking and the function of the lacrimal sac. The outer aspect of the muscle is mainly run by the zygomatic branch and is recruited during voluntary forceful lid closure.
The ORL, also known as the orbitomalar ligament, is a circumferential osteocutaneous ligament arising from the periosteum of the orbital rim, and, in the lower lid, it traverses the orbicularis oculi between the preseptal and preorbital portions to insert into the dermis of the lid-cheek junction. Medially, it is tightly bound to the periosteum and creates the inferior aspect of the nasojugal groove, or tear trough. This ligament can be released in the preperiosteal plane to smooth the lid-cheek junction and facilitate the mobility of the midface. Furthermore, this area often exhibits one of the earliest signs of facial aging and can be effectively treated with fillers to blend the transition from the lid to the cheek.
The middle lamella consists of the orbital septum and is the landmark anatomic structure separating the inner and outer layers.
The orbital septum is a delicate, but distinct, fascial structure of the eyelid, which inserts directly onto the caudal edge of the tarsal plate. It is continuous with the periorbital periosteum and can be surgically followed as a plane to the midface periosteum. The septum serves as the anterior boundary containing the fat pads of the eye.
The lower lid has 3 intraorbital fat pads, lateral, central, and medial. They are managed in different ways to improve lid-cheek aesthetics. The lateral and central fat pads are separated by the arcuate expansion of Lockwood ligament, which inserts into the orbital rim anterolaterally. The central and medial fat pads are separated by the inferior oblique muscle, the injury of which will cause diplopia.
The posterior lamella (the innermost layer of the eyelid closest to the globe) of the lower eyelid consists of the tarsal plate, lower lid retractors, and the conjunctiva.
The tarsal plate is a dense fibrous structure almost 1 mm thick at the superior aspect of the lower eyelid giving structure to the lid margin. In the lower lid, it is approximately 4 to 5 mm tall. It contains meibomian glands, which secrete the lipid layer of tear film. ,
The lower lid retractors are a combination of muscle and fascial tissue that displaces the lower lid downward. The inferior tarsal muscle is a layer of smooth muscle that joins with the orbital septum and becomes a common ligament referred to as the capsulopalpebral fascia that inserts into the inferior tarsal border. When looking down, the inferior rectus muscle contracts, as do the lower lid retractors, retracting the lower lid to open the lower visual field. Cutting the lower lid retractors allows the lower lid margin to rise upward. ,
The palpebral conjunctiva on the inner surface of the eyelid reflects onto the globe at the fornix to become the bulbar conjunctiva. Everting the lower lid, one will notice 2 vascular arcades: one overlying the tarsus, and one just above the fornix. These 2 arcades serve as useful markers during surgery when deciding where to place a transconjunctival incision.
Preoperative evaluation
A history and examination focusing on the eye and eyelid function are an important part of the preoperative work up before lower eyelid surgery. , , ,
One should note a history of hypertension and any anticoagulant medications, as these factors can increase the risk of postoperative hematoma. Preoperative visual acuity is recorded. A history of dry eye symptoms, or refractive/LASIK surgery within the last 6 months, predisposes patients to dry eye, exposure, and corneal complications. If dry eye is a consideration, these patients should undergo a Schirmer test to evaluate adequate tear production, and/or tear film breakup time to evaluate for evaporative dry eye disease.
A thorough functional lower lid evaluation is very important and involves an evaluation of laxity with a lower lid distraction test (>0-mm distraction from the globe being the sign of significant laxity) and of orbicularis tone with a snap-back test. The snap test is positive if after the lid is distracted it does not reassume contact with the globe until a blink has occurred. If either finding is present, the need for a canthal tightening procedure is considered. Objectively, lower lid tone and scleral show should be evaluated by the margin reflex distance-2 (MRD2), the distance from pupillary light reflex to the lower lid margin. This distance should be less than 5 mm. The presence of the protective Bell phenomenon (globe rotates cephalad when the eyelids close) is noted, as an absence increases the risk of postoperative exposure keratitis.
Evaluation of the midface and globe position will help identify a preoperative predisposition to postoperative lower lid malposition. Patients with a negative vector (malar eminence lies posterior to the anterior-most point of the cornea on lateral view) are prone to lower lid malposition because of a relative deficiency of midface support. Patients with a prominent globe, measured with a Hertel exophthalmometer, are more likely to develop lower lid malposition if surgery is not carefully planned to account for this.
In addition to these functional considerations, patients are evaluated for the extent of lower lid fat pseudoherniation, lower lid skin excess, presence of a tear trough deformity, and degree of midface aging. To evaluate the degree of herniated fat, the patient looks upwards while the surgeon palpates the lid-cheek junction. Alternatively, the surgeon can gently press on the globe when the patient’s eyes are closed, accentuating the pseudoherniated fat. The degree of midface aging is assessed by evaluating the lid-cheek junction, looking for skeletonization of the inferior orbital rim and making note of any malar bags or lateral edema.
Indications for transconjunctival blepharoplasty
The key to successfully treating the signs of aging of the lower eyelid and lid-cheek junction using the transconjunctival blepharoplasty lies in proper patient selection. , In patients with pseudoherniated fat, mild to moderate skin excess, and mild to moderate lid-cheek junction skeletonization, a variety of techniques can be combined with the transconjunctival approach. The typical candidate who is best for a transconjunctival approach is the one with prominent fat pads as the dominant feature of the lower lids. Patients with skin and muscle laxity may be good candidates for this approach; however, the degree of aesthetic improvement begins to diminish with more signs of aging. Therefore ancillary procedures, such as skin pinch, skin resurfacing, and/or fat repositioning, will maximize aesthetic outcomes. Of course, the other option is to select more invasive lower lid procedures; however, these will extend recovery times and increase morbidity.
Preoperative planning
Skin Management
Skin pinch
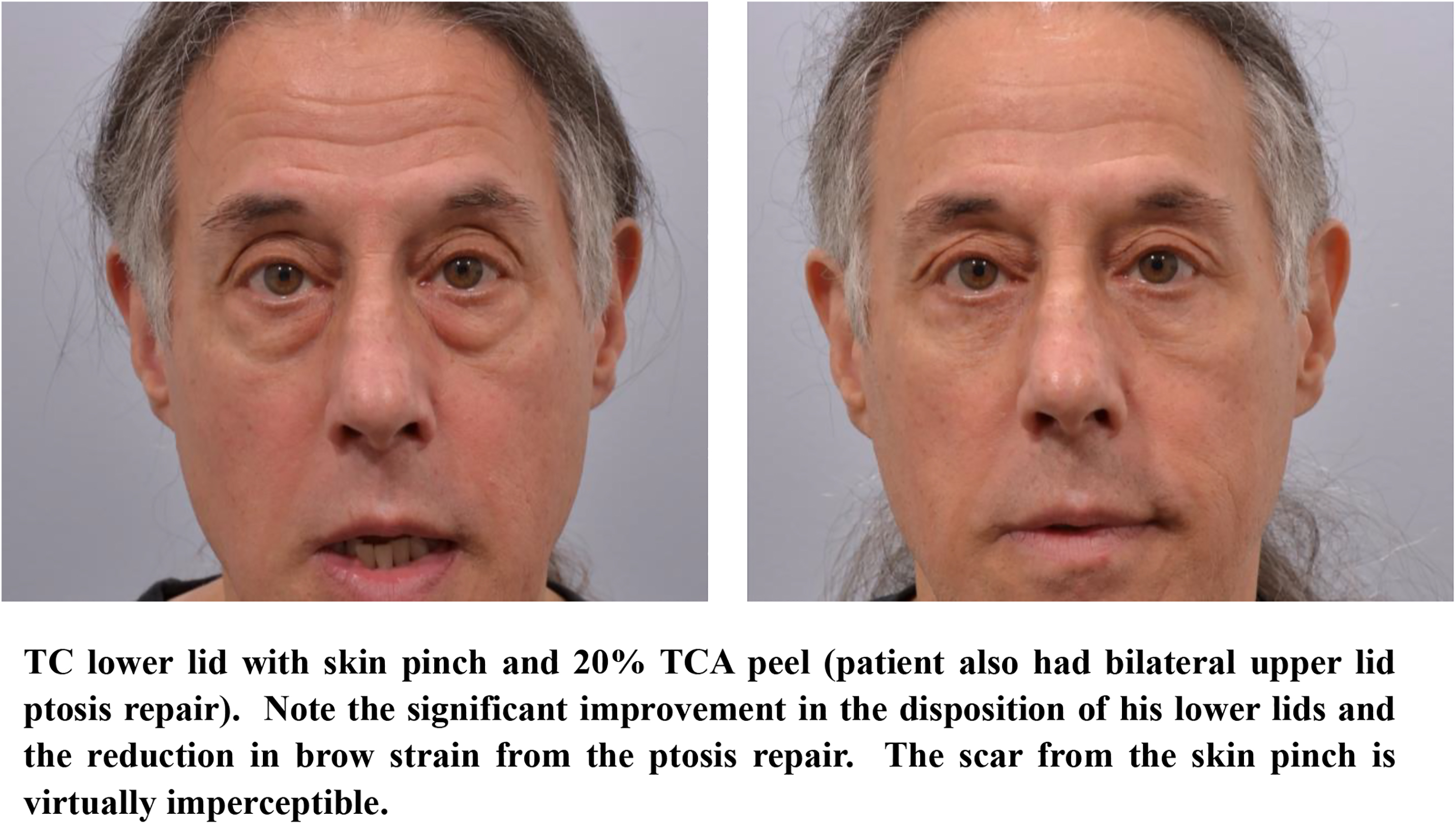
A skin pinch technique, when performed concomitantly with transconjunctival blepharoplasty, can be used to manage mild lower eyelid skin excess with the use of a subciliary skin-only incision. This skin pinch technique preserves the orbicularis muscle and avoids middle lamellar scarring, with the nominal downside of adding a virtually imperceptible subciliary scar. Properly performed, this technique yields a stable postoperative lower eyelid position (no change in MRD2) when compared with a transconjunctival blepharoplasty without skin pinch. If performing a skin pinch and an upper lid blepharoplasty, ensure that there are at least 6 mm of skin between the lateral limbs of the 2 incisions (see clinical case example; Fig. 2 ).
Skin undermining
A skin-only flap of the lower lid with conservative skin resection at the level of a subciliary incision can also be used to manage excess skin of the lower lid with transconjunctival blepharoplasty.
This “inside-outside” approach, which releases the attachments between orbicularis muscle and lower eyelid skin, was touted by Hidalgo as superior in skin-smoothing potential when compared with the skin pinch technique. Using this approach, Hidalgo demonstrated lower lid malposition in only 3 of 248 consecutive patients. Similarly, Rosenberg and colleagues showed no postoperative difference in MRD2 or lateral canthal rounding using this approach in 78 consecutive patients.
Skin resurfacing
To improve lower eyelid skin quality or dyschromia, skin resurfacing with peels or lasers can be used in conjunction with a transconjunctival blepharoplasty. Resurfacing is typically performed on the face as a whole to prevent demarcation, but the lower lid is an exception and can be treated alone with little risk of demarcation. (See clinical case example; Fig. 2 ). A survey study of current practice trends among active American Society of Ophthalmic Plastic and Reconstructive Surgery members reported the use of laser skin resurfacing by 36% of the members and chemical peels by 29% of responding members.
For laser or chemical skin resurfacing, it is important to realize that patients with Fitzpatrick skin types IV, V, and VI are at increased risk of developing dyspigmentation or hypertrophic scarring after treatment. For these patients, treatment should be limited to superficial peels if indicated. Typically, the darker the skin, the less severe the photoaging, and therefore, less need for resurfacing.
Skin preparation for a chemical peel includes 4 weeks of topical tretinoin, hydroquinone, and sun protection, all of which should be resumed once reepithelialization has occurred. For patients with a history of cold sores, herpes prophylaxis should begin 1 day preprocedure and continue for 4 days postprocedure.
Medium-depth peels, such as a 20% to 30% TCA, are especially effective in improving advanced photoaging in the periorbital area. Deeper chemical peels, such as a 0.1% croton oil peel, can better address deeper rhytides. The senior authors most commonly use croton oil for skin resurfacing of the lower eyelid in their practice. However, deeper peels are also associated with more potential complications, including risk of scarring, textural changes, prolonged erythema, hyperpigmentation or hypopigmentation, and risk of ectropion. If an ectropion does develop and is not due to the surgical technique or midlamellar scarring, it tends to be self-limiting and corrects with conservative care.
Laser resurfacing of the lower eyelid can improve texture and dyschromia and provides some skin tightening. Skin preparation is minimal, primarily requiring that the patient be diligent with sunblock and avoiding tanning. Antiherpes prophylaxis is recommended. Multiple options exist, including ablative devices, nonablative and radiofrequency devices, and fractional devices. It is important to note that ablative lasers, particularly the ablative co 2 , carry a higher risk of lower eyelid ectropion, particularly in patients undergoing secondary blepharoplasty. Clinical studies have shown that the ablative Er:YAG laser, although more superficial in penetration when compared with the co 2 laser, is effective for both superficial and deep rhytides in the lower eyelid, probably owing to the thin skin in this area. Segal and colleagues combined transconjunctival blepharoplasty with erbium laser resurfacing without inducing lid retraction.
Whichever resurfacing modality is chosen, the most important factor in avoiding complications and obtaining good results is operator comfort and proficiency with a given technique.
Fat management
The transconjunctival approach allows the surgeon to address herniated orbital fat as well as midface volume loss. In manipulating the inferior orbital fat pads, a surgeon has options, including excision alone, augmentation with autologous fat grafts, or fad pad transposition.
Fat Resection
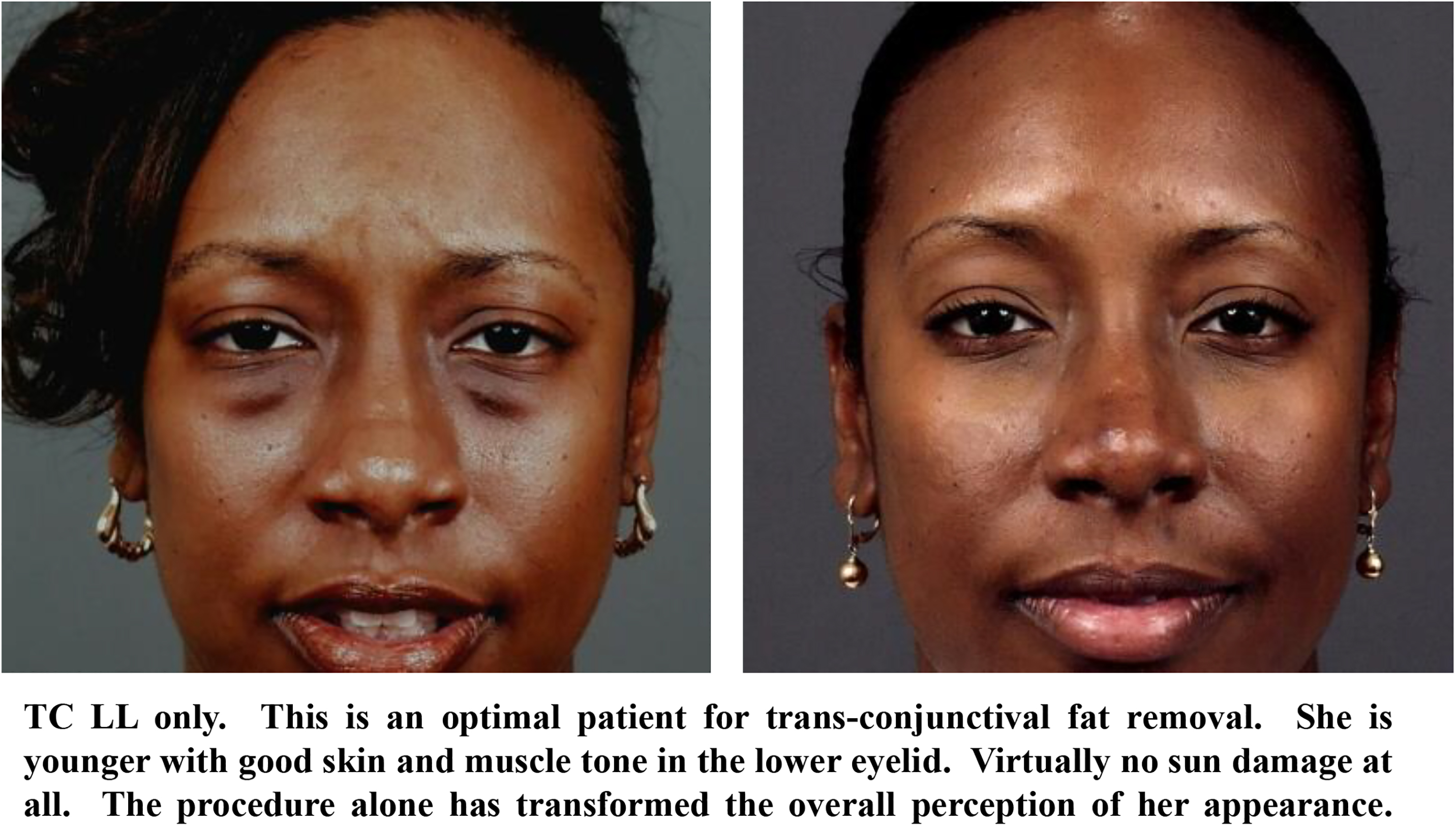
For patients with isolated lower lid bags, little or no skin excess, and no inferior orbital rim volume loss, a transconjunctival approach to resecting the lower lid fat is potentially all that is needed. The transconjunctival approach is rarely associated with lower lid malposition and often has the added benefit of decreasing scleral show without a concomitant canthal procedure. This is due to the incision through the lower lid retractors allowing elevation of the lower lid. When fat is resected, it should be done in all 3 compartments, and as a general rule, is trimmed back to the point where it is flush with the orbital rim (see clinical case examples; Figs. 3–5 ).
Related posts:
 Treatment Options for Lower Eyelid Festoons
Treatment Options for Lower Eyelid Festoons
 Blepharoptosis Repair: External Versus Posterior Approach Surgery: Why I Select One over the Other
Blepharoptosis Repair: External Versus Posterior Approach Surgery: Why I Select One over the Other
 The Treatment of Post-blepharoplasty Lower Eyelid Retraction
The Treatment of Post-blepharoplasty Lower Eyelid Retraction
 My Evolution with Endoscopic Brow-Lift Surgery
My Evolution with Endoscopic Brow-Lift Surgery
 Transcutaneous Blepharoplasty with Volume Preservation
Transcutaneous Blepharoplasty with Volume Preservation
 Periorbital Fat Grafting
Periorbital Fat Grafting
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


