The endoscopic approach for forehead rejuvenation and brow lift has many advantages. It provided excellent exposure for release of periorbital soft tissues combined with endoscopic magnification, shorter scars, and reduced risk of alopecia and scalp sensory changes compared with the traditional open coronal brow lift. The technique has improved over the last 15 years with better fixation devices, a better understanding of the longevity, and decreased complications of the procedure. The endoscopic brow lift offers the patient a much easier and safer solution for the aging forehead, active wrinkles from corrugator and frontalis hyperactivity, and the ptotic, asymmetric brow.
Key points
- •
Brow aesthetics and surgical options for brow lift and forehead rejuvenation.
- •
Ideal candidates for the endoscopic brow-lift technique.
- •
Forehead and periocular anatomy.
- •
Surgical technique and the 4 key steps for endoscopic brow rejuvenation.
- •
Long term results and complications.
Introduction
The endoscopic approach for forehead rejuvenation and brow lift has many advantages. It provided excellent exposure for release of periorbital soft tissues combined with endoscopic magnification, shorter scars, and reduced risk of alopecia and scalp sensory changes compared with the traditional open coronal brow lift. The technique has improved over the last 15 years with better fixation devices, a better understanding of the longevity, and decreased complications of the procedure. The endoscopic brow lift offers the patient a much easier and safer solution for the aging forehead, active wrinkles from corrugator and frontalis hyperactivity, and the ptotic, asymmetric brow.
Content
Indications
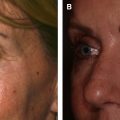
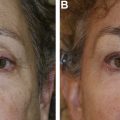
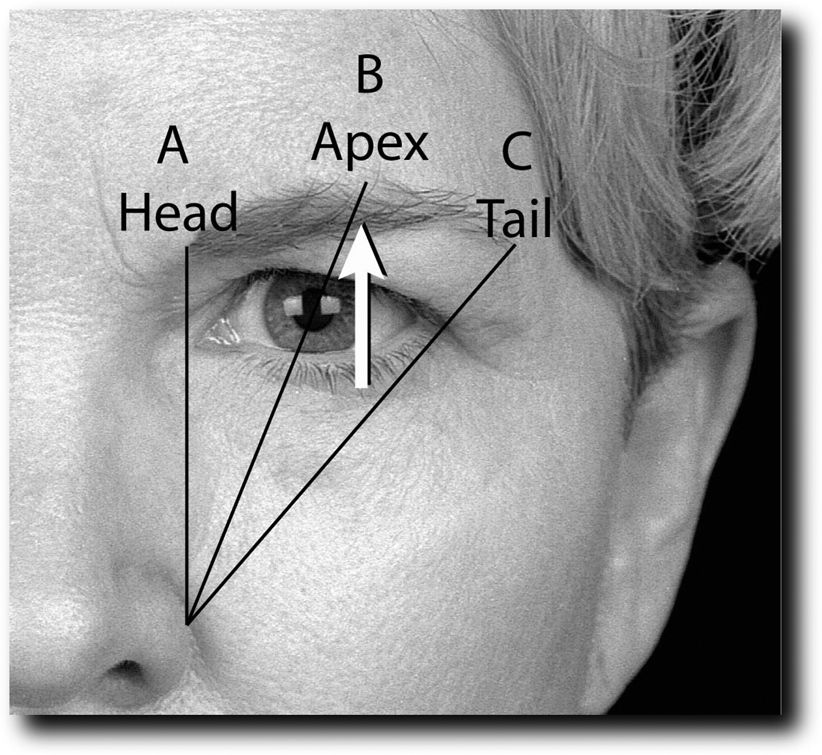
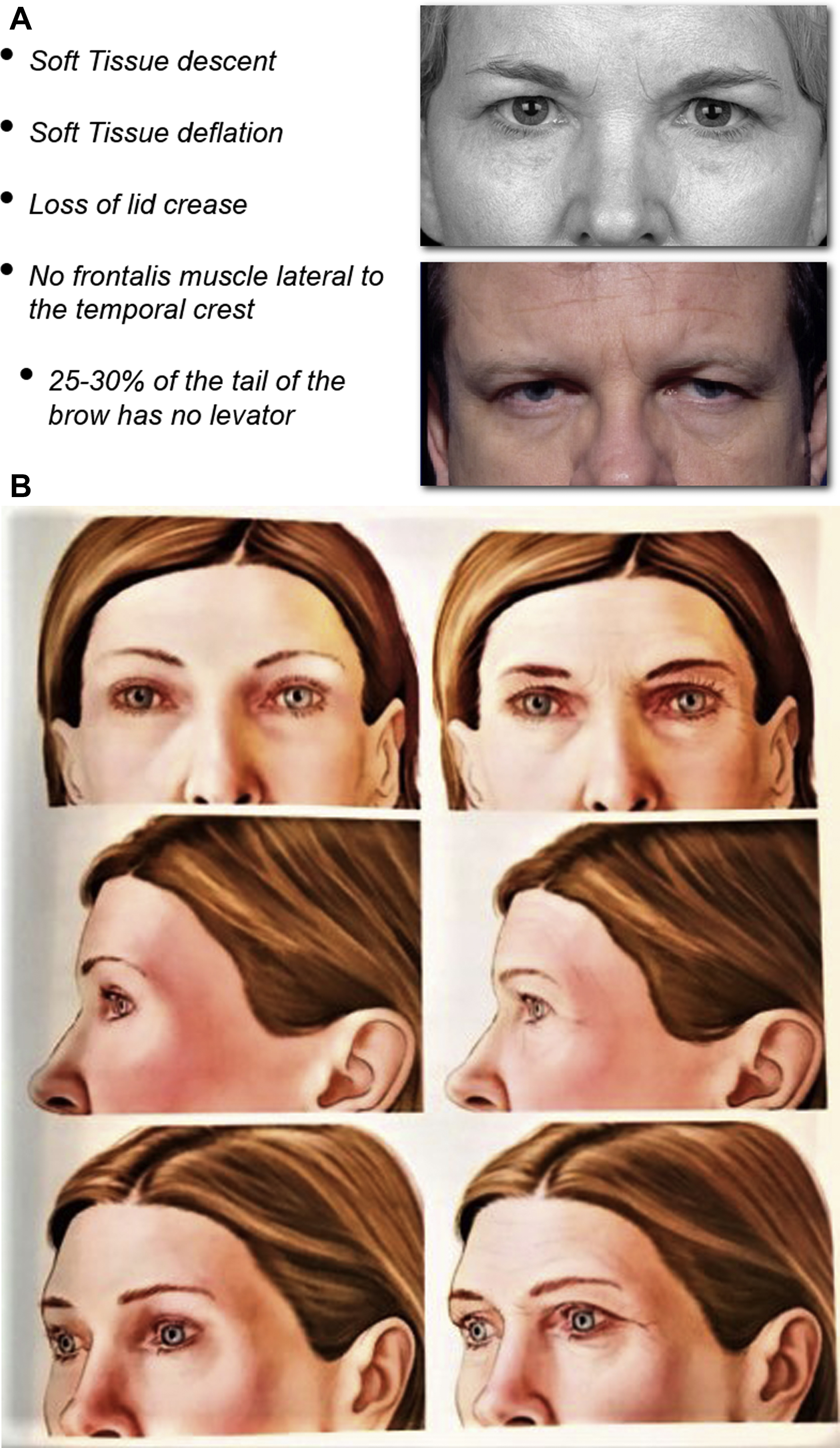
The generally accepted ideal for the shape and position of the brow has been changing over the years and through different cultures; therefore, brow aesthetics cannot be generalized and must be evaluated in relation to gender, ethnicity, orbital shape, culture, and overall facial aging and proportions. Currently, we consider the “ideal aesthetic brow” with the medial brow at or below the level of the orbital rim, above the medial canthus, and with a gentle peak on the last two-thirds toward the lateral end with the lateral tail higher than the medial ( Fig. 1 ). Men’s brows should be straight and located at the level of the supraorbital rim with no lateral temporal elevation, which is a characteristic of the female brow. With facial aging, the eyebrows gradually fall and lose volume, encroach on the orbit, and bunch the skin over the lateral orbital rim, creating what is known as “temporal hooding.” Anatomically, there is no levator mechanism on the lateral brow allowing tissue ptosis and loss of volume for causing the lateral or temporal brow ptosis. Eyebrow ptosis, eyebrow asymmetry, temporal hooding, and forehead wrinkles are all indications for forehead rejuvenation and a brow lift ( Fig. 2 ).
Patient Selection
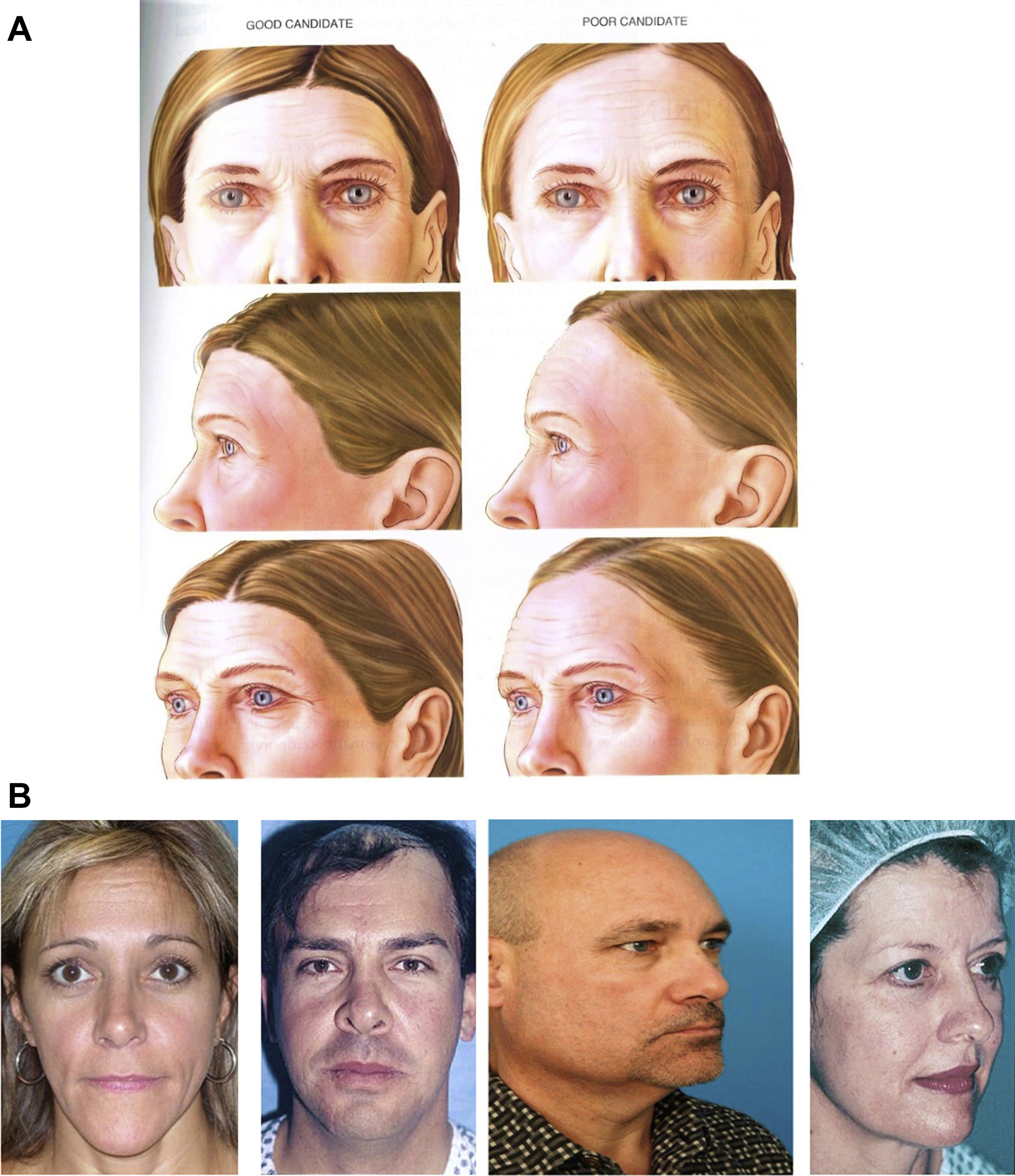
Techniques for forehead rejuvenation include open coronal, lateral temporal brow lift, direct approach through the brow, transpalpebral brow lift with direct excision of the corrugator muscles, endoscopic brow lift, and neurotoxin injections. Since the introduction of the endoscopic approach to brow lift in 1993 by Vasconez and Core, I have not performed an open coronal brow lift. Almost all of my facial rejuvenation cases today include forehead and brow rejuvenation through an endoscopic technique. The best candidates for endoscopic forehead rejuvenation and brow lifts are patients with flat foreheads (flat frontal bone), no receding hairline (low hairline), and minimal redundant forehead skin. High hairlines and male-pattern baldness add to the challenge of being able to see and remove the glabellar muscles and achieve fixation. In patient selection, the key problems to be addressed are eyebrow ptosis, eyebrow position, brow asymmetry, hyperactive frontalis and corrugator muscles, and frontal and glabellar frown lines.
Anatomy (Brief Review)
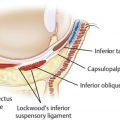
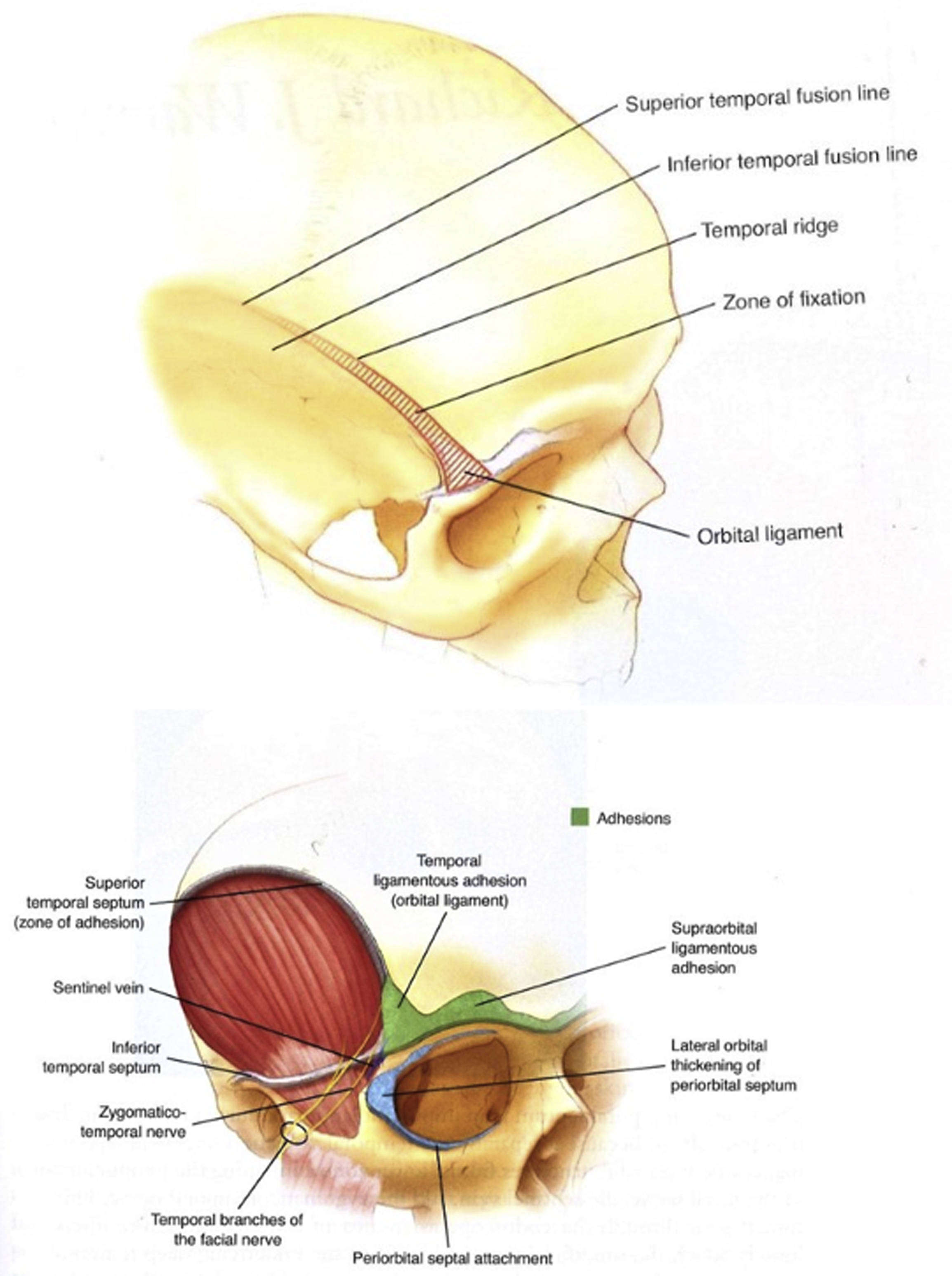
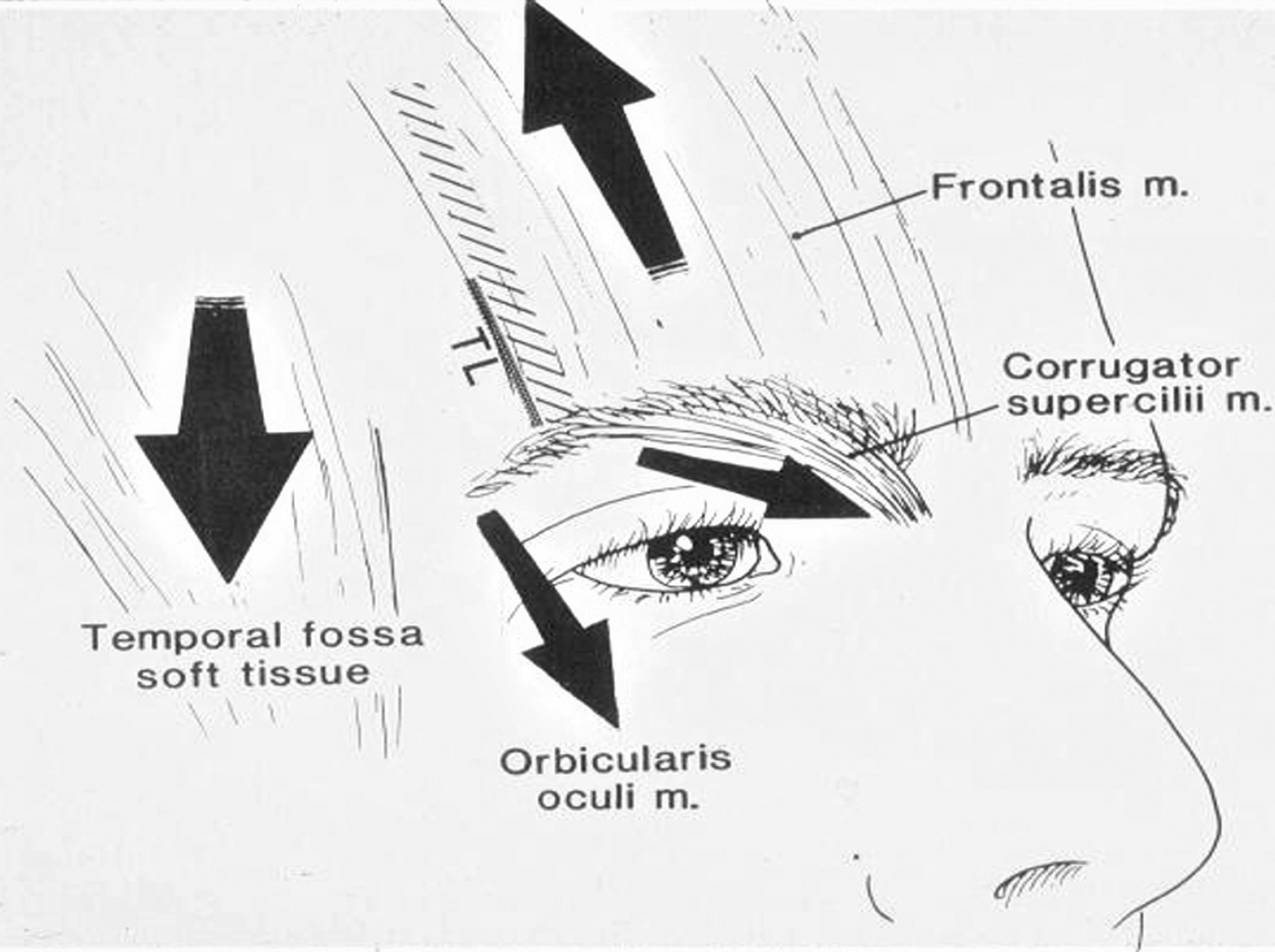
The anatomy of the forehead and periorbital regions should be appreciated by the surgeon. The temporal ridge is bound by the temporal line of fusion, which is a deep bony point of fixation of the overlying soft tissue. The junction of the facial bone periosteum with the deep temporal fascia is what is known as the temporal fusion line. It is most caudal extension named fusion ligament. In order to adequately release and mobilize the lateral brow and temporal region, the temporal line of fusion should be released to the level of the supraorbital rim. There are also supraorbital ligamentous attachments that require release in order to elevate the brow and forehead soft tissues ( Fig. 3 ).
The nerves that are encountered and preserved during endoscopic brow lift include the supratrochlear and supraorbital nerves, the 2 main sensory nerves, and the frontal nerve, the main motor branch of the facial nerve. Care is taken to appreciate and preserve these nerves during dissection. Subgaleal dissection (below superficial temporal fascia) lateral to the temporal line of fusion will maintain the plane of dissection deep to the frontal branch. Inferior dissection to the level of the sentinel vein while remaining the dissection superficial to the deep temporal fascia protects the frontal branch from direct division or traction neuropraxia (injury). Appreciation that the neurovascular bundles for the supratrochlear and supraorbital nerves exit the orbit 1.5 and 2.5 cm from midline, respectively, allows gentle division of the periosteum at that location to avoid division of the associated vascular bundles or damage to the nerves ( Fig. 4 ).
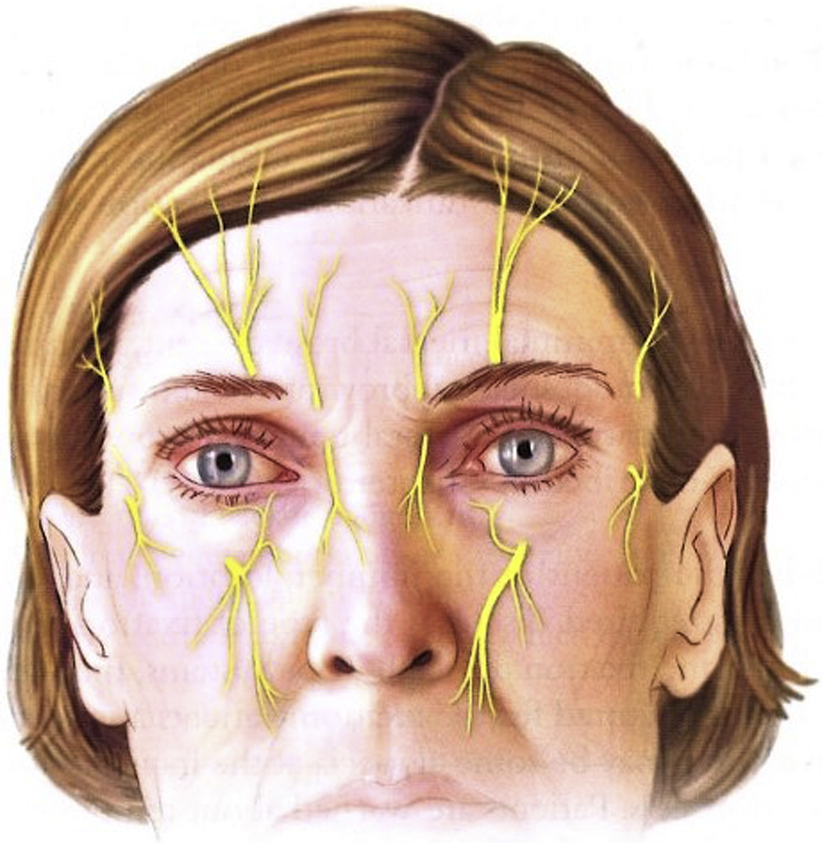
The sentinel vein is inferior to the inferior temporal septum and approximates the level of the frontal branch for the facial nerve.
The muscles of the forehead include the frontalis, procerus, corrugator supercilii (with oblique and transverse heads), the depressor supercilii, and the orbicularis muscles. The brow elevator is the frontalis muscle, whereas the other muscles all act in various fashions as brow depressors. Although release and physical repositioning of the brow and forehead elevate the brow, division and weakening of the brow depressors also correct dynamic brow ptosis and glabellar frown lines ( Fig. 5 ).
Preoperative Preparation
Assessment of the patient includes evaluation of both the medial and the lateral brow position, the ratio from brow to upper eyelid, glabella and forehead lines, forehead shape and height, and the hairline shape and position. To assess the strength of the muscle action, movement, and depth of soft tissue folds, the patient should be asked to frown as well as to raise the eyebrows. The eyebrows should also be assessed for the thickness, shape, position, and symmetry. In preoperative consultation, the doctor should advise as to the number of incisions and type of fixations. Based on the patient assessment, the operation can be planned. Patient inclusion is important in that brow lifts are individualized. The preoperative evaluation in front of a mirror with input from the patient is key for a successful outcome and reasonable expectations. The discussion and markings should focus on possible elevation of the anterior hairline; medial brow elevation; position, shape, and elevation of the lateral brow; softening and spreading of the intermedial brow space after corrugator resection ( Fig. 6 ).
The endoscopic technique is based on the use of modern technology whereby the traditional eye-hand surgical coordination is done through a video-endoscopic system. Additional extensive training is necessary not only for the surgeon but also for all medical and nursing personnel involved in the surgical case. The novice should take his or her first assistant to cadaver workshops and/or courses to learn together. The equipment, from endoscope to camera and monitors, is usually standard in centers where aesthetic surgeries are performed. It has become important to test each system, inspect each instrument, and check for a backup system as a safeguard. The surgeon must have knowledge of the principles extending from training, equipment needs and operation, and technical skills.
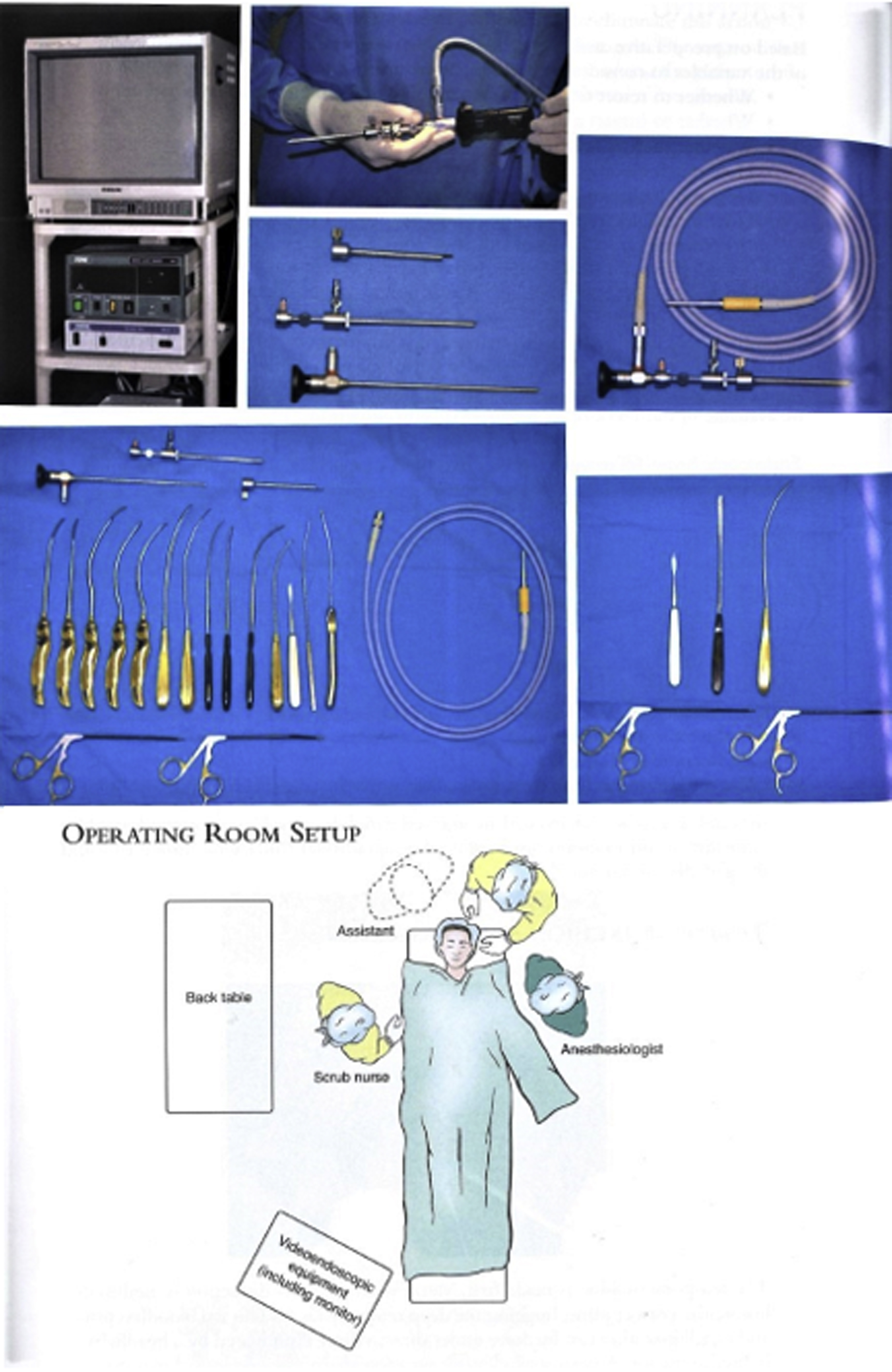
Equipment
Although use of the endoscopic brow lift has nearly eliminated the need for open coronal brow lifts, there are additional equipment requirements. Equipment should be tested before induction of anesthesia, and backup equipment should be available. The endoscopic equipment on the cart for visualization includes a monitor (preferably high definition), a 3-chip camera with the ability to record the procedure digitally and take still photographs, light source, electrocautery base unit, and suction. The additional equipment on the field should include an endoscope (most commonly a 4- to 5-mm 30-degree Hopkins rod with an endoscopic sheath), camera connector, light source connector, endoscopic dissectors, endoscopic forceps, endoscopic scissors, endoscopic graspers, and a malleable Durden suction cautery. The devices used for fixation can include a drill for a cortical tunnel, a drill for temporary screw fixation, a drill for use of the Endotine device (MicroAire, Charlottesville, Virginia, USA), or a variety of other fixation methods preferred by the surgeon. The endoscopic cart should be positioned at the foot of the bed with the surgeon positioned at the head of the bed ( Fig. 7 ).