Fig. 11.1
Face is divided into horizontal thirds. The upper third extends from the hairline to glabella, the middle third from glabella to subnasale, and lower third from subnasale to menton
However, even if the vertical proportion of the face is ideal, the face may look longer depending on the ratio of the width-to-height ratio of the face. In general, the width-to-height ratio of the face is typically 3:4, with an oval-shaped face being the aesthetic ideal [1, 2]. Therefore, long faces are highly subjective; the indications for surgery cannot be absolute. For example, some Koreans or Japanese people having normal range of chin in good proportion sometimes want shorter chin. Moreover, the lower face, which is shorter than the ideal proportion, is recognized as a younger face in Asian countries [3, 4]. Surgeon needs to know exactly what the patient wants to improve through careful consultation and should take comprehensive consideration of various factors to improve the long face effectively and harmoniously.
In this chapter, authors focus on the improvement of a long face using shortening of soft tissue for the midface and vertical reduction of the mandible for a lower face.
For the shortening of the midface, as is well known, the only way to shorten actual length and correct malocclusion is double-jaw surgery adopting Le Fort I osteotomy. However, patients who have (1) normal or near-normal occlusion or who do not want correction of occlusion, (2) who want less invasive surgery and quick recovery, and (3) who have concomitant redundant soft tissue (philtrum) with minimal incisor show philtrum reduction surgery is an effective and alternative method of making the midface look shorter.
For the shortening of lower face, facial contouring surgeries such as mini V-line surgery and V-line surgery adopting T-shape osteotomy for reduction genioplasty are the most common and effective methods. Furthermore, control of soft tissue along with shortening of the vertical length of the mandible is a very important factor in lower face shortening. As redundant soft tissue still make shortened mandible after facial bone contouring surgery look still longer, suspension of soft tissue such as geniohyoid/digastric muscle, liposuction, and face lifting should be considered.
Patient Assessment and Consultation
Direct physical examinations and clinical photos are the key processes to evaluate the patient’s problems and establish a surgical plan. Cephalometric/panoramic radiographs and three-dimensional computed tomography are also necessary. Among them, the lateral cephalogram is a profile X-ray of the skull and soft tissues and is most useful to assess the vertical proportions and the relation of the soft tissues to the jaws. Although there is no absolute definition of long faces as mentioned above, it is worthwhile to consider aesthetic “ideals” when analyzing the face preoperatively and making a surgical plan.
For the midface, patients having long and thin upper lip with the incisor show of less than 2 mm and hooding of the lateral lip are good candidates for the philtrum reduction.
Considering the ideal facial for reference and patients’ demand, surgeons decide which operation would be applied to shorten the long face.
Surgical Techniques
Facial Bone Contouring Surgeries: V-Line and Mini V-Line Surgery
Surgical techniques are not far different from prevalent facial bone contouring surgeries described at previous chapters. The major difference is the axis of osteotomy and additional osteotomy for vertical shortening. Various osteotomy designs can be considered depending on the position of the nerve, the amount of reduction, and the patients’ needs.
Two Parallel Osteotomy
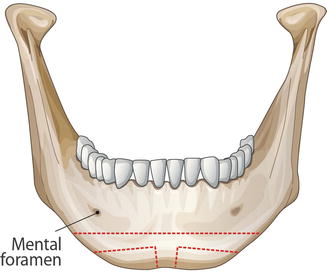
Chin shortening using two parallel osteotomy lines is a commonly used technique when the nerve runs high enough or amount of reduction is not so much. This method is technically an easy and time-saving method as surgeons can make two parallel osteotomy lines with double-bladed saws. These parallel osteotomy lines may be applied horizontally, but it may also be applied as an inverted V shape to obtain additional shortening effects (Fig. 11.2). If the location of the nerve is too low to limit the reduction and if the risk of subsequent nerve injury is likely to increase, or if the patient wants the maximum pointed chin with a reduction in length, surgeons should consider safe and alternative osteotomy line.
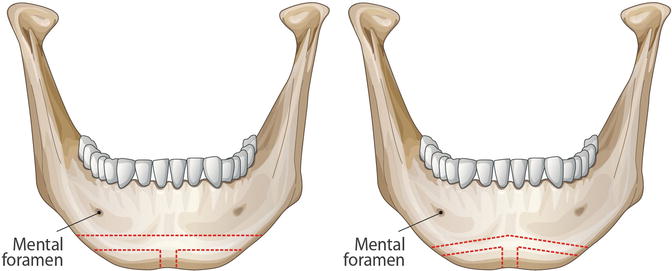
Fig. 11.2
Two parallel osteotomy. It is most commonly used reduction technique
Inverted V-Shape Osteotomy
In cases where the position of the inferior alveolar nerve line is too low, if there is not enough margin to the nerve line due to the previous operation, and if only a small degree of vertical reduction is required, the length of the chin can be reduced through oblique deformation of the osteotomy line without removal of the bone (Fig. 11.3). Although the amount of vertical reduction is limited, it is the most commonly used method of osteotomy because the risk of nerve damage is relatively low and the method of osteotomy is simple and not technically challenging as it is not much different from the transverse osteotomy. In general, to maintain the shape of the chin, it is necessary to remove the central strip, which is twice the amount of vertical reduction.
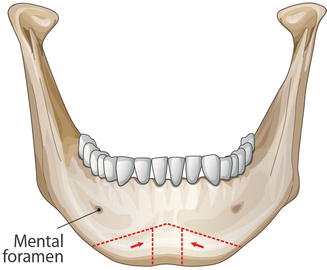
Fig. 11.3
Inverted V-shape osteotomy. Length of the chin can be reduced through oblique deformation of the osteotomy line without removal of the bone
Trapezoidal-Shape Osteotomy
If the patient does not prefer a pointed chin and wants a round chin and a maximum length reduction, osteotomy should focus mainly on shortening (Fig. 11.4). By maximally removing the bones in the central portion and minimally removing the bones at both ends, the length of the chin can be reduced sufficiently even if the position of the nerve is low.
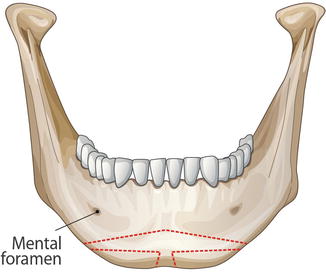
Fig. 11.4
Trapezoidal-shape osteotomy. It enables maximum length reduction
Bow-Tie-Shape Osteotomy
If the patient’s chin is not too long and the patient wants shorter but more pointed chin, the purpose can be done through combination of transverse and oblique osteotome line (Fig. 11.5). The design of osteotomy is opposite to that of trapezoidal-shape osteotomy. By minimally removing the bones in the central portion and maximally removing the bones at both ends, a more pointed chin can be achieved although the reduction of length is somewhat limited. However, when using bow-tie-shape osteotomy, there should be enough space for the nerve line as there would be a lot of bony steps at both ends.