Fig. 10.1
Surgical procedures of the mini V-line surgery
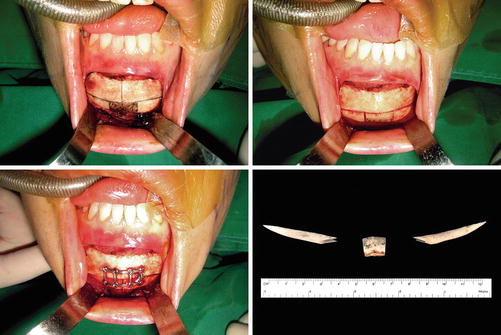
Fig. 10.2
Intraoperative photographs of the mini V-line surgery. A horizontal osteotomy line and two vertical osteotomy lines are designed (top left). Osteotomies are carried out with a reciprocating saw (top right). After removing the middle bone segment, the two lateral bony segments are fixed with a microplate and screws in the center (bottom left). Bone segments removed during surgery (bottom right)
Narrowing of the chin leaves a bony step on each side of the chin-mandible junction, and this discontinuity should be diminished to reduce its palpability and for a smooth jaw line. Additional lateral incisions are made alongside the previous intraoral incision that was made for the chin narrowing procedure. These incisions are separated from each other because exposing the mental nerve increases the incidence of direct nerve injury during the operation. Subperiosteal dissection is then performed through the newly made lateral incisions to obtain direct visual access medially from the chin-mandible junction and laterally to the mandible angle. The use of a “guarded” oscillating saw to mark the proposed osteotomy line is recommended (Fig. 10.3) [10, 14]. This guarded saw has a small oscillating saw that is shielded at various distances. The size of the guarded saw to use is determined by the size of the bony step (which correlates with the amount of chin narrowing) and the distance between the lower mandible border and route of the nerve. The saw allows the surgeon to perform a precise bone resection in a uniformed manner while avoiding over-resection and reducing the possibilities of nerve injury. The extent of the ostectomy should be extended to a point posteriorly to allow a smooth jaw line. This point can be in the middle of the mandible body or just anterior to the gonion, depending on the shape of the mandible, the steepness of the mandible plane, and the amount of chin narrowing. If the posterior extent of the resection is too short, an unnatural and unsmooth jaw line, namely, a “secondary angle,” may form, resulting in an unaesthetic outcome [10]. After the osteotomy line is marked with the guarded saw, larger oscillating saws are serially used to complete the bone resection. Additional mandibular corticectomy can be performed if further narrowing of the width of the mandible body is required (Fig. 10.4).
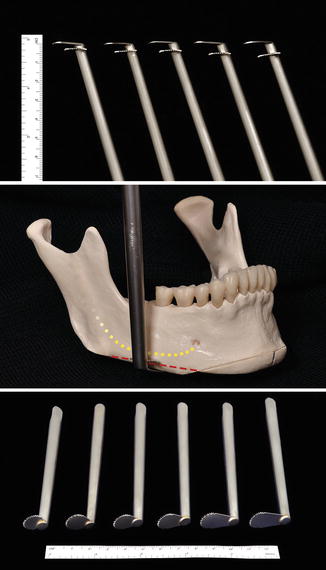

Fig. 10.3
The use of “guarded” oscillating saws. The guarded saw has a small oscillating saw that is shielded at various distances: 2, 3, 4, 5, and 6 mm (top). The saw helps the surgeon to perform the bony resection precisely while avoiding over-resection and nerve injury (middle). Further bone resections are completed by serial use of larger oscillating saws (bottom)
Fig. 10.4
Preoperative panoramic radiograph (left). Follow-up radiograph 1 day after surgery (right)
Key Technical Points
- 1.
During the T-osteotomy procedure for chin narrowing, the horizontal osteotomy should be perpendicular to the facial midline and at least 5 mm inferior to the mental foramen.
- 2.
The width of the central chin narrowing portion is determined based on factors such as the wideness of the chin, the course of the inferior alveolar nerve, and the patient’s preferences. According to the authors’ clinical experience, the average amount of horizontal narrowing was about 10 mm, ranging from 0 to 16 mm.
- 3.
Anteroposterior adjustment of the chin or vertical chin lengthening or shortening procedure can be carried out simultaneously with the chin narrowing procedure.
- 4.
It is important to smoothen the bony step on each side of the chin-mandible junction and reduce its palpability. The bony steps are reduced by using oscillating saws. The “guarded” oscillating saw leads to a precise bony resection in a uniform fashion while avoiding over-resection and reducing the possibilities of nerve injury.
Case Study
Case 1
A 26-year-old woman was planned for the mini V-line surgery. Although her mandible angles were not very prominent with a gonial angle of 130°, the accentuated chin broadness gave her a rather masculine appearance. The chin was narrowed by 10 mm and simultaneously vertically shortened by 2 mm to achieve good facial proportions. Additional upper blepharoplasty was performed concomitantly. Her relatively broad lower face had a more slender and feminine postoperative contour after surgery (Fig. 10.5).

Fig. 10.5
 Essential Surgical Anatomy for Facial Bone Contouring Surgery
Essential Surgical Anatomy for Facial Bone Contouring Surgery
 The Mini-Zygoma Reduction Surgery
The Mini-Zygoma Reduction Surgery
 Surgical Approaches for Facial Bone Surgery
Surgical Approaches for Facial Bone Surgery
 Alloplastic Augmentation of the Midface
Alloplastic Augmentation of the Midface
 Treatment of Long Face with Facial Bone Contouring Surgery and Philtral Reduction
Treatment of Long Face with Facial Bone Contouring Surgery and Philtral Reduction
 Secondary and Revisional Zygoma Reduction
Secondary and Revisional Zygoma Reduction




Preoperative view of a 26-year-old woman (left). Postoperative view at 6 months after mini V-line surgery (right)
Related posts:
Essential Surgical Anatomy for Facial Bone Contouring Surgery
The Mini-Zygoma Reduction Surgery
Surgical Approaches for Facial Bone Surgery
Alloplastic Augmentation of the Midface
Treatment of Long Face with Facial Bone Contouring Surgery and Philtral Reduction
Secondary and Revisional Zygoma Reduction
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
