Fig. 2.1
The course of inferior alveolar nerve and mental nerve. The inferior alveolar nerve is the largest branch of the mandibular division of the trigeminal nerve (CN V) and carries sensory and motor fibers. The IAN travels through the inferior alveolar canal which is positioned at a variable vertical height. The mental nerve exits the mental foramen that is located midway between the alveolar and basal borders of the mandible and is usually below or slightly anterior to the second premolar tooth
The mental nerve provides sensation to the skin and mucosa of the lower lip, the skin in the region of the chin, and the facial gingiva of the anterior teeth. The mental nerve exits the mental foramen that is located midway between the alveolar and basal borders of the mandible and is usually below or slightly anterior to the second premolar tooth. The mental nerve divides under the depressor anguli oris muscle into three main branches; one descends to the skin of the chin, and the other two ascend to the skin and mucous membrane of the lower lip and gingiva [4].
Infraorbital Nerve (Fig. 2.2)
The most important neurovascular structure that must be negotiated during procedures in the midfacial region is the infraorbital neurovascular bundle. The infraorbital nerve is the largest cutaneous branch of the maxillary division of the trigeminal nerve (CN V). The artery and vein that accompany the infraorbital nerve are surgically insignificant. The nerve exits the infraorbital foramen, 7–10 mm inferior to the infraorbital rim just medial to the zygomaticomaxillary suture, or approximately at the medial and middle thirds of the orbit [3]. After exiting the infraorbital foramen, the infraorbital nerve divides into terminal branches that spread fanlike into the lower eyelid, nose, and upper lip. Three of the four superior labial branches enter the lip between its muscles and the mucous membrane. These nerves supply not only the mucous membrane of the upper lip, but also its skin, which they reach by perforating the orbicularis oris muscle. Damage to this nerve results in loss of sensation in these areas, and possibly dysesthesia. Therefore surgeon should check the location of infraorbital foramen before surgery and pay attention in order not to irritate the nerve during surgery, especially malar reduction or malar augmentation surgery using implants. In malar reduction surgery, the position of plate and screws should be determined after confirmation that they won’t disturb the infraorbital nerve. Because proximity of plate and screws to the foramen can cause irritation to the nerve, plate should be cut in case of too narrow space between the nerve and osteotomy line. In augmentation malarplasty using implant, the implant should be trimmed and positioned carefully in order not to compress or disturb the infraorbital nerve.
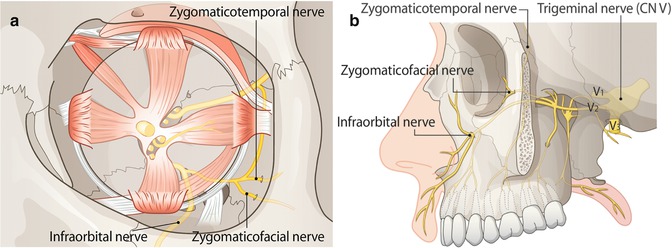
Fig. 2.2
Infraorbital nerve, zygomaticofacial nerve, and zygomaticotemporal nerve. ((a) Frontal view (b) Lateral view) The infraorbital nerve is the largest cutaneous branch of the maxillary division of the trigeminal nerve (CN V). After exiting the infraorbital foramen, the infraorbital nerve divides into terminal branches that spread fanlike into the lower eyelid, nose, and upper lip. The zygomaticotemporal and zygomaticofacial nerve pierce the periorbital sac, traverse the opened subperiosteal space, and exit the orbit laterally. They innervate sensation to the skin over their distribution in the area of the lateral orbital margin and the prominence of the zygomatic body
Zygomaticotemporal/Zygomaticofacial Nerve (Fig. 2.2)
During the dissection of the inferior portion of the lateral orbital wall, two branches of the sensory zygomatic nerve (branch of V2), the zygomaticotemporal and zygomaticofacial nerve, are identified. They pierce the periorbital sac, traverse the opened subperiosteal space, and exit the orbit laterally. The zygomaticotemporal nerve can ascend in a groove on the lateral orbital wall and will enter a canal in the orbital surface of the zygoma, leading to the temporal fossa. The zygomaticofacial nerve also runs through a canal in the zygoma and exits laterally over the prominence of the zygomatic body.
The subperiosteal dissection of the lateral orbital wall from an inferior access usually requires division of these two sensory branches of the zygomatic nerve, causing loss of sensation to the skin over their distribution in the area of the lateral orbital margin and the prominence of the zygomatic body [5]. In malar reduction surgery, these two nerves can be damaged during dissection or ostectomy resulting in about a coin-sized insensate area near the lateral orbit. Therefore careful dissection should be made near the lateral orbit to identify these nerves and preserve them if it is possible.
Facial Nerve (Fig. 2.3)
The main trunk of the facial nerve (CN VII) emerges from the skull base at the stylomastoid foramen. It lies medial, deep, and slightly anterior to the middle of the mastoid process at the lower end of the tympanomastoid fissure. After giving off the posterior auricular and branches to the posterior digastric and stylohyoid muscles, it passes obliquely, inferiorly, and laterally into the substance of the parotid gland. It divides into the temporofacial and cervicofacial divisions at a point vertically below the lowest part of the bony external auditory meatus. The terminal branches of the facial nerve emerge from the parotid gland and radiate anteriorly. They are commonly classified as temporal (frontal), zygomatic, buccal, marginal mandibular, and cervical. Among these, the temporal branch and the marginal mandibular branch are significant because they might be injured during facial bone contouring surgeries.
Fig. 2.3




Facial nerve, artery, and vein. The main trunk of the facial nerve (CN VII) emerges from the skull base at the stylomastoid foramen. The terminal branches of the facial nerve emerge from the parotid gland and radiate anteriorly. They are classified as temporal (frontal), zygomatic, buccal, marginal mandibular, and cervical. The facial artery originates from the external carotid artery, grooving or passing through the submandibular salivary glands as it rounds the lower border of the mandible. It is visible on the external surface of the mandible around the anterior border of the masseter muscle. The facial vein begins as the angular vein, courses along with the facial artery above the level of the inferior mandibular border. The facial vein runs across the surface of the submandibular gland to end in the internal jugular vein
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
