Fig. 3.1
Maxillary vestibular approach. The body of the zygomatic bone can be easily approached through an intraoral incision without leaving external scars. The dissection ranges superomedially to the infraorbital neurovascular bundle (a), superolaterally to the lateral edge of the infraorbital rim and laterally behind the zygomaticomaxillary buttress (b)
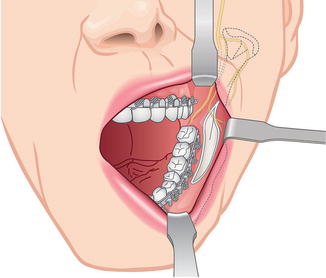
Fig. 3.2
Mandibular vestibular approach. The intraoral incision is the main surgical approach for a mandible contouring surgery. Superb visualization and access is possible while leaving no external scars and violating the facial motor and sensory nerves
Bicoronal Approach
The bicoronal approach can be used to expose the skeleton of the upper and middle face. During a facial bone contouring surgery, the bicoronal approach may be performed for a malar reduction procedure or for a forehead contouring. First of all, the hairline of the patient must be considered when designing the line of incision. The incision may be curved anteriorly at the vertex, paralleling but remaining 5 cm within the hairline. Bicoronal incisions with a zigzag design may be used to make the scars less noticeable. The bicoronal incision can be extended inferiorly to the level of the earlobe with extension by a praeauricular incision. This approach allows direct exposure of the zygomatic arch and the infraorbital rims.
Bleeding from the incision site can be reduced by injecting vasoconstrictors into the proposed incision line. Incision is made with a scalpel extending from one superior temporal line to the opposite side. The incision is deepened pass through the skin, subcutaneous tissue and galea, revealing the subgaleal plane of loose areolar tissues which overlies the pericranium. The flap can be easily lifted and dissected above the pericranium. The skin incision below the superior temporal line should extend to the depth of the superficial layer of the temporalis fascia and into the subgaleal plane which has continuity with the dissection above the superior temporal line.
After elevation of the anterior and posterior wound margins by 1–2 cm, haemostatic Raney clips may be applied or bleeding vessels may be isolated and electrocauterized. Extensive cauterization of the edge of the incision sites damages the hair follicles and produces alopecia. The flap may be elevated above the pericranium with manual finger dissection, with blunt periosteal elevators. On the lateral aspect of the skull, the temporalis fascia becomes visible as it merges with the pericranium at the superior temporal line. The plane of dissection is just superficial to this thick fascia. Once the flap has been dissected anteriorly and inferiorly several centimetres, it should be possible to evert the flap so that the galeal is superficial. If it is not possible to evert the flap, further dissection inferiorly along the superficial layer of the temporalis fascia, and possibly extending the skin incision more inferiorly, may be necessary. Dissection of the flap continues anteriorly in the subgaleal fascial plane until 3–4 cm superior to the supraorbital rim. A horizontal incision is made through the pericranium from one superior temporal line to the other. The subperiosteal dissection then continues downward to the supraorbital rims. The lateral portion of the flap is dissected inferiorly above through the temporalis fascia. As the dissection extends inferiorly near the ear, the superficial layer of temporalis fascia is incised at the root of the zygomatic arch, just in front of the ear. The incision continues anterosuperiorly to join the cross-forehead incision previously made through the pericranium at the superior temporal line. Dissection made inferiorly should be just deep to the superficial layer of the temporalis fascia. This layer provides a safe route of access to the zygomatic arch because the temporal branch of the facial nerve is always lateral to the superficial layer of the temporalis fascia. Blunt scissors are used to dissect just under the superficial layer of the temporalis fascia. Once the superior surface of the zygomatic arch and the posterior border of the body of the zygoma are visible, an incision is made through the periosteum along their superior surface. The incision is continued superiorly along the posterior border of the body of the zygoma and the orbital rim, ultimately meeting the cross-forehead horizontal incision through the pericranium. Then the subperiosteal elevation totally exposes the lateral surfaces of the zygomatic arch, the body of the zygoma and the lateral orbital rim.
When closing the bicoronal incision, suture resuspension of the soft tissues is recommended. Closure of the periosteum around the orbital rims is performed with absorbable sutures. The scalp incision is closed in two layers using absorbable sutures through the galea and subcutaneous tissues and non-absorbable skin sutures or staples (Fig. 3.3) [1–3].
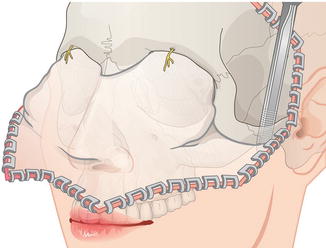
Fig. 3.3
Bicoronal approach. The bicoronal approach is performed to directly expose the upper and mid face skeleton. Especially, full access to the zygomatic body and arch and the lateral and inferior orbital rims is possible
Transcutaneous Approach
- 1.
Sideburn approach
An incision can be made on the sideburn area for direct access to the posterior portion of the zygomatic arch. At the level of the zygomatic arch, an 8–10 mm length incision should be made with a scalpel on the midline of the sideburn. The incision is deepened carefully as the incision site is adjacent to the frontal branch of the facial nerve. For such reasons, blunt dissection for the subcutaneous fatty layer is recommended rather than cutting by electrocautery or sharp scissors. When the dissection is deepened to the periosteal layer of the zygomatic arch, a sharp incision is made on the periosteum. Then using a periosteal elevator, subperiosteal dissection is continued for exposure of the osteotomy and fixation site. Later for wound closure, absorbable sutures should be done at two points for the subcutaneous layer, followed by simple non-absorbable sutures for skin closure (Fig. 3.4) [4, 8].
- 2.
Gillies’ approach
The Gillies’ approach describes a temporal incision made 2.5 cm superior and anterior to the helix, within the hairline. As a 2 cm length temporal incision is made, care is taken to avoid the superficial temporal artery. Then the dissection continues through the subcutaneous tissue and superficial temporal fascia down to the deep portion of the deep temporal fascia. This fascia is then incised to expose the temporalis muscle. Through this plane, a periosteal elevator is inserted deep to the temporalis fascia and superficial to the temporalis muscle. Using a back-and-forth movement of the elevator, the elevator is advanced until the posterior portion of the zygomatic body is reached. Later for wound closure, the scalp can be simply closed with staples (Fig. 3.5) [4].