Patients with facial paralysis require a systematic zonal assessment. One frequently overlooked region is the effect of facial paralysis on nasal airflow. Patients with flaccid paralysis experience increased weight of the cheek and loss of muscle tone in the ala and sidewall; this significantly contributes to nasal valve narrowing and collapse. These specific findings are often not adequately corrected with traditional functional rhinoplasty-grafting techniques. Flaccid paralysis typically results in inferomedial displacement of the alar base, which must be restored with suspension techniques to fully treat the nasal obstruction. Multiple surgical options exist and are discussed in this article.
Key points
- •
Nasal obstruction is a common symptom associated with facial paralysis yet often is overlooked.
- •
The fundamental discrepancy causing nasal obstruction in patients with flaccid paralysis versus nonflaccid paralysis is inferomedial displacement of the alar base.
- •
Nasal valve suspension produces superolateral displacement of the ala and is necessary for correcting nasal obstruction in flaccid paralysis.
- •
The authors’ nasal valve suspension technique uses marginal and temporal incisions with fascia lata to produce reliable results without external facial scars.
Introduction
Patients with facial paralysis require a systematic zonal assessment to assure no areas are overlooked. Flaccid paralysis results from denervation of muscles of facial expression and leads to facial asymmetry from loss of tone and increased skin laxity. One frequently overlooked region is the effect of facial paralysis on nasal airflow. It is important to distinguish flaccid and nonflaccid facial paralysis when assessing nasal obstruction. Patients with nonflaccid paralysis, such as incomplete paralysis with or without synkinesis, typically respond well to cartilage-grafting techniques performed in rhinoplasty. Patients with flaccid paralysis experience increased weight of the cheek as well as loss of muscle tone in the ala and sidewall; this significantly contributes to nasal valve narrowing and collapse. These specific findings are often not adequately corrected with traditional functional rhinoplasty-grafting techniques. Successfully treating nasal obstruction in the setting of facial paralysis begins with a thorough history and physical examination. Flaccid paralysis typically results in inferomedial displacement of the alar base, which must be restored with suspension techniques to fully treat the nasal obstruction. Multiple surgical options exist and are discussed in this article.
Anatomy
The term nasal valve was first introduced by Mink in 1903 and was further described in detail by Bridger and Proctor in 1970. , The internal nasal valve comprises the caudal edge of the upper lateral cartilage, the septum, the head of the inferior turbinate, and the soft tissue overlying the piriform aperture. The internal nasal valve angle is created by the caudal edge of the upper lateral cartilage and the septum; this angle should measure 10° to 15° but varies with ethnicity. The internal nasal valve is the narrowest portion of the nasal cavity and contributes at least 50% of nasal airflow resistance. The external nasal valve is the area delineated by the nostril rim. Medially, it is defined by the medial crus of the lower lateral cartilage and columella. Inferiorly, it is bound by the nasal sill and floor of the nose. Laterally, the external valve consists of the alar sidewall.
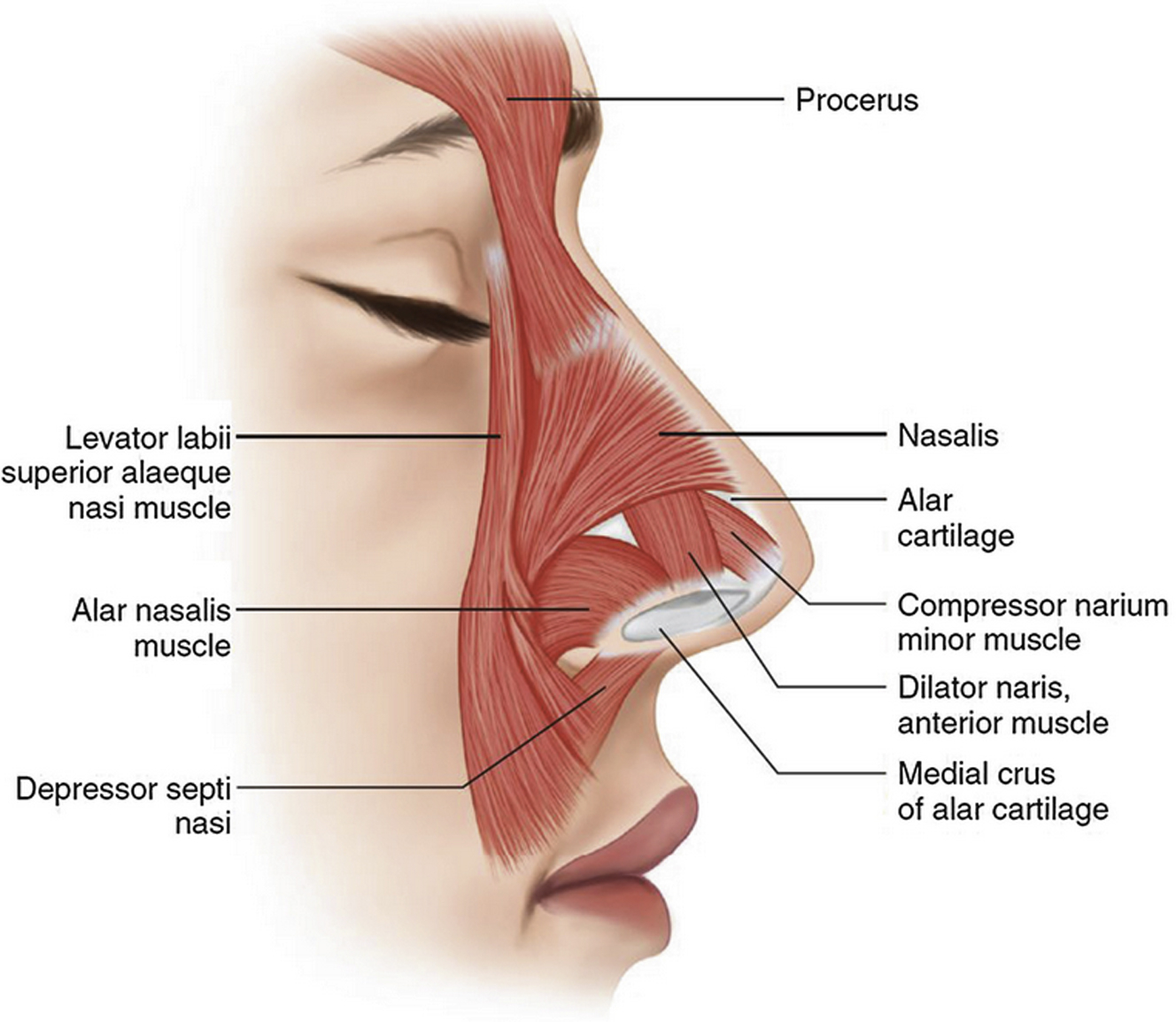
The alar sidewall is commonly referred to as the “fibrofatty tissue of the ala”; this is the most compliant portion of the nose because of lack of cartilage support. However, there is significant muscle activity that supports and stents the nasal ala and sidewall. The dilator naris muscle occupies a large majority of the ala and plays an important role in opening and strengthening the external valve. The alar portion of the nasalis muscle (pars alaris) inserts on accessory cartilage and influences lateral stability of the ala. The transverse portion of the nasalis (pars transversalis) does not directly insert onto the nasal cartilage but stabilizes the nasal valve and sidewall while acting on the nasal skin , ( Fig. 1 ).
An additional important structure within the alar subunit is the piriform ligament. The piriform ligament is a fibrous ligamentous attachment that extends from the lateral crura to the piriform crest. This structure provides further stability to the alar sidewall; however, it may act as a limiting factor when surgically widening the alar base. This retaining ligament can be divided for complete mobilization.
Physiology
The nose acts as a dynamic airflow resistor. As inspired air enters the nose, the airflow travels superiorly, and its speed increases 5-fold within the internal nasal valve. This region makes up for 50% or more of the total airway resistance. The airflow becomes turbulent, enhancing warming and humidification. Posterior to the nasal valve, the airflow decreases to approximately its entrance speed and turns horizontally and then inferiorly toward the choanae. The airflow becomes laminar and increases speed as it enters the nasopharynx.
Nasal airflow follows the principle explained by Bernoulli. A liquid or gas flowing through a tube increases its velocity and diminishes the transmural pressure at an area of constriction. The Bernoulli effect explains why the nasal valve collapses at varying degrees of nasal inspiration. Three factors determine the amount of nasal valve collapse with inspiration: the shape of the nasal valve area, the cross-sectional area of the nasal valve, and the integrity of the nasal sidewall and ala. Poiseuille’s law states that flow is inversely related to the radius to the fourth power, which explains why a slight decrease is nasal valve area results in a dramatic decrease in nasal airflow.
Evaluation of nasal obstruction
When evaluating patients with facial paralysis, a systematic approach should be implemented. When focusing on nasal obstruction, a thorough history focusing on the nasal symptoms will help one determine the fundamental problem. Understanding the effect of nasal obstruction on the patient’s quality of life is important to determine the appropriate management option. Patient-based quality-of-life surveys focusing on facial palsy (Facial Clinimetric Evaluation Scale, Facial Disability Index) and on nasal obstruction (Nasal Obstruction and Septoplasty Effectiveness Scale) should be obtained.
The nasal examination begins with external inspection. Careful attention is paid to the frontal view, examining for any asymmetry, particularly at the alar insertion. Flaccid facial paralysis may result in inferior and medial displacement of the ala on the paretic side. Palpation of the middle third of the nose is helpful in determining the width of the internal valves. On the base view, the position of the columella, medial footplates, and caudal septum are all inspected. Again, alar base width and asymmetry are noted. Anterior rhinoscopy is performed next, with careful inspection of the septum, inferior turbinates, and internal and external valve area. Observation of the middle meatus and view of the middle turbinate should be noted. The shape and overall surface area of the external valve are observed. Lateral crura position and evidence of medial recurvature are also noted.
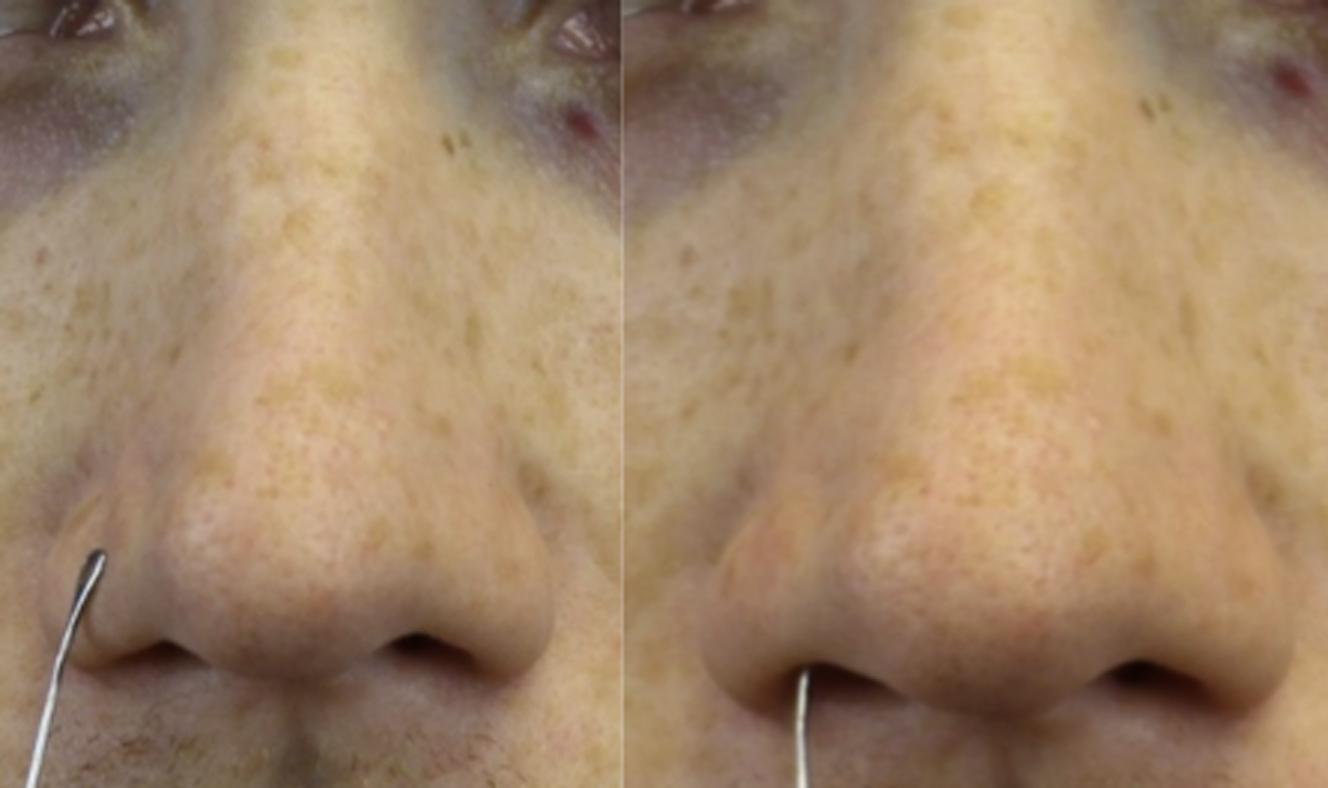
Returning to the base view, the dynamic examination is performed. The patient is asked to breathe normally through the nose while one observes for dynamic nasal sidewall collapse and medial movement of the alar base. The modified Cottle maneuver is performed next in the external valve position or the area of most significant collapse. First, the lateral wall is merely stabilized in position, and normal inspiration is resumed while noting the patient’s findings. Next, the lateral wall is lateralized approximately 1 mm and results are recorded ( Fig. 2 ). The modified Cottle maneuver is then performed in the internal valve area ( Fig. 3 ). The modified Cottle maneuvers are more specific for changes achieved with functional rhinoplasty grafts. Last, the Cottle maneuver, superolateral displacement of the patient’s cheek, is performed, and the findings are recorded ( Fig. 4 ). Typically, flaccid paralysis patients’ symptoms are more significantly improved with this maneuver, as this addresses the inferomedial displacement of the alar base.

Related posts:
 Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
 Modified Selective Neurectomy
Modified Selective Neurectomy
 Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
 Dual Nerve Transfer for Facial Reanimation
Dual Nerve Transfer for Facial Reanimation
 Dual Innervation of Free Functional Muscle Flaps in Facial Paralysis
Dual Innervation of Free Functional Muscle Flaps in Facial Paralysis
 Facial Reanimation and Reconstruction of the Radical Parotidectomy
Facial Reanimation and Reconstruction of the Radical Parotidectomy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


