Radical parotidectomy may result from treating advanced parotid malignancies invading the facial nerve. Survival is often enhanced with multimodality treatment protocols, including postoperative radiation therapy. In addition to the reconstructive challenge of restoring facial nerve function, patients may be left with a significant cervicofacial concavity and inadequate skin coverage. This should be addressed with stable vascularized tissue that is resistant to radiation-induced atrophy. This article describes a comprehensive strategy, includes the use of the anterolateral thigh free flap, the temporalis regional muscle transfer, motor nerve to vastus lateralis grafts, nerve to masseter transfer, and fascia lata grafts for static suspension.
Key points
- •
A comprehensive reconstructive approach is required to address the challenges posed by radical parotidectomy, which include rehabilitation of facial paralysis, restoration of facial volume, contour, and symmetry, and attainment of adequate skin coverage.
- •
Although nerve grafting procedures may provide for optimal facial reanimation, dynamic regional muscle transfer may offer immediate facial symmetry and some expressive movement. Combined approaches of dynamic and static procedures aim to restore immediate facial resting symmetry during or in the absence of reinnervation.
- •
The anterolateral thigh is a versatile and rich reconstructive donor site that can provide modifiable vascularized soft tissue volume restoration, skin coverage, nerve grafts, and fascia lata grafts for facial reanimation procedures.
Introduction
Total parotidectomy with facial nerve sacrifice (radical parotidectomy) is performed to treat as many as 20% of parotid gland malignancies when the facial nerve is invaded by a tumor. In addition to facial paralysis, removal of these tumors often leaves patients with significant soft tissue defects of the lateral face and neck and loss of skin coverage. In many cases, postoperative radiation is required to treat these aggressive tumors and should be taken into account when planning the reconstruction. The top priorities for facial reanimation are corneal protection and maintenance of oral competence, followed by restoration of resting symmetry and finally the attainment of dynamic movement. The options for facial reanimation are myriad and include nerve transfer, nerve interposition grafting, static suspension, local muscle transposition, and free tissue transfer. Although reinnervation usually provides the best functional outcomes, its effects may not be noticeable for up to 6 to 12 months. ,
In general, microvascular free flap reconstruction improves blood flow and promotes wound healing in the recipient wound bed, leading to stable soft tissue volumes that are resistant to radiation-induced atrophy. As a part of the oncologic resection, a cervical lymphadenectomy is often performed, providing exposure and access to donor blood vessels for microvascular anastomosis. Additionally, mastoidectomy or lateral temporal bone resection may be necessary because of tumor invasion and/or the need to gain negative surgical margins on proximal perineural tumor spread. It is the authors’ preference to approach the reconstruction of the radical parotidectomy defect using a comprehensive approach that starts with the use of the anterolateral thigh (ALT) free flap. This flap offers several key advantages:
Stable and easily modifiable vascularized tissue volume for contour correction,
Vascularized skin for additional cutaneous coverage if needed
Access to tensor fascia lata that can be used for static suspension
Access to the motor nerve to vastus lateralis (MNVL) for cable grafting
Efficiency of a 2-team approach for simultaneous tumor extirpation and flap harvest
Performing an orthodromic temporalis tendon transfer (OTTT) at the time of resection can provide patients with immediate dynamic facial symmetry while awaiting reinnervation. A comprehensive approach also includes performing smaller procedures that address the other consequences of facial paralysis including brow ptosis, lagophthalmos, and ectropion.
Facial nerve reconstruction and reanimation
A recent analysis of the National Surgical Quality Improvement Program (NSQIP) database revealed that concurrent facial reanimation and extirpative surgery are performed infrequently, with rates between 24% and 31%. , It is common practice to defer facial reanimation until after the completion of adjuvant treatment. However, several studies have demonstrated that postoperative radiation and positive nerve margins do not necessarily correlate with adverse nerve reconstruction outcomes. Facial reanimation undertaken at the same setting of the extirpation is encouraged, when possible, as facial nerve branches are more easily identified for nerve grafting or nerve transfer, and the duration of facial paralysis and denervation atrophy of facial mimetic muscles are reduced. ,
Nerve Grafting
Depending on the extent of facial nerve resection during a radical parotidectomy, it is usually not feasible to perform a primary coaptation of the proximal and distal nerve segments in a tension-free manner. In these cases, interposition sensory or motor nerve grafts may be used as a method of reinnervation. , Outcomes do not appear to be significantly affected by adjuvant radiation therapy; patients who underwent nerve grafting and radiation therapy did not have statistically significant outcomes to those who underwent nerve grafting without postoperative radiation. , , Some of the more commonly used nerve grafts include the MNVL, cervical sensory nerve, sural nerve, great auricular nerve, lateral antebrachial cutaneous nerve (LCAN), and the anterior division of the medial antebrachial cutaneous nerve (MACN). , , In earlier animal studies, motor nerves grafts appeared to be better suited for motor nerve regeneration compared with sensory nerve grafts. It was hypothesized that this difference is caused by closer matching of the size of the Schwann cell basal lamina tubes, which are larger in motor nerves than in sensory nerves, allowing a greater number of nerve fibers to cross the nerve graft coaptation. , However, a recent study has refuted this claim and demonstrated equivalent outcomes across 4 validated metrics for motor and sensory nerve grafts in a mouse model. Further research is required to achieve consensus and determine if it also translates clinically. In cases where a suitable nerve graft is not available or to avoid donor site morbidity, cadaveric allografts may be indicated and offer similar outcomes for the reconstruction of sensory, motor, and mixed nerve deficits from 5 to 50 mm.
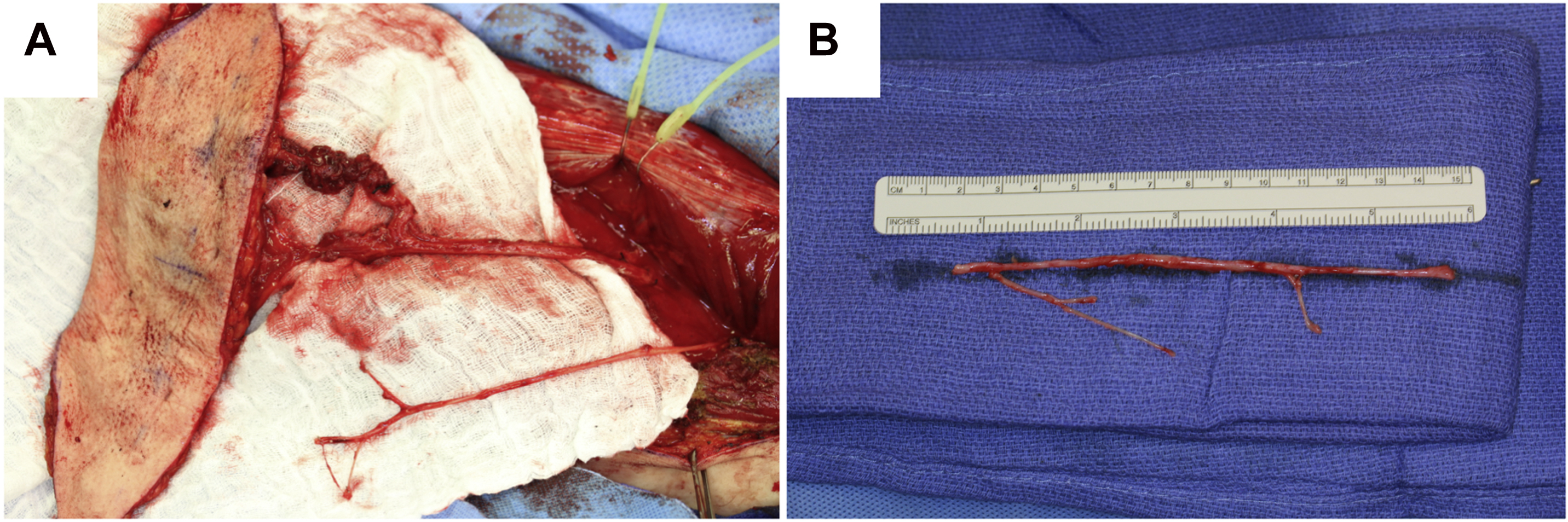
Functional recovery is optimized when the nerve gap occurs distal to the pes anserinus, with subsegmental grafting minimizing synkinesis. When the proximal facial nerve is available for nerve grafting, retrograde orientation of the nerve grafts is usually encouraged to minimize axonal escape via regenerating nerves being lost at branch points. However, it is technically difficult to coapt multiple strands to a single facial nerve stump. The MNVL averaged 9.4 cm in length (range 5.1–19.6 cm), and had an average of 4.4 branches, each of which has a mean of 2.3 secondary branches, as shown in a cadaveric study. In vivo, multiple branches (3–5) can often be identified, each of which may be coapted to a distal nerve. This permits efficient single nerve coaptation to the facial nerve trunk, which can then be coapted to multiple distal nerves. For this reason, even when employing the masseteric nerve transfer to the buccal or zygomatic division, the authors encourage the use of the MNVL as an interposition graft during radical parotidectomy. The MNVL is conveniently accessible during an ALT free flap harvest ( Fig. 1 ), as the nerve virtually always accompanies the course of the descending branch of the lateral circumflex artery and vein. The MNVL is easily dissected free from the vascular pedicle and has minimal to no associated morbidity because of the apparent redundant innervation of the vastus lateralis. This nerve would be difficult to access for pure nerve grafting procedures in a patient not undergoing an ALT free tissue transfer surgery, as the incision for access would need to be long and the required dissection complicated and time consuming.
Nerve to Masseter Transfer
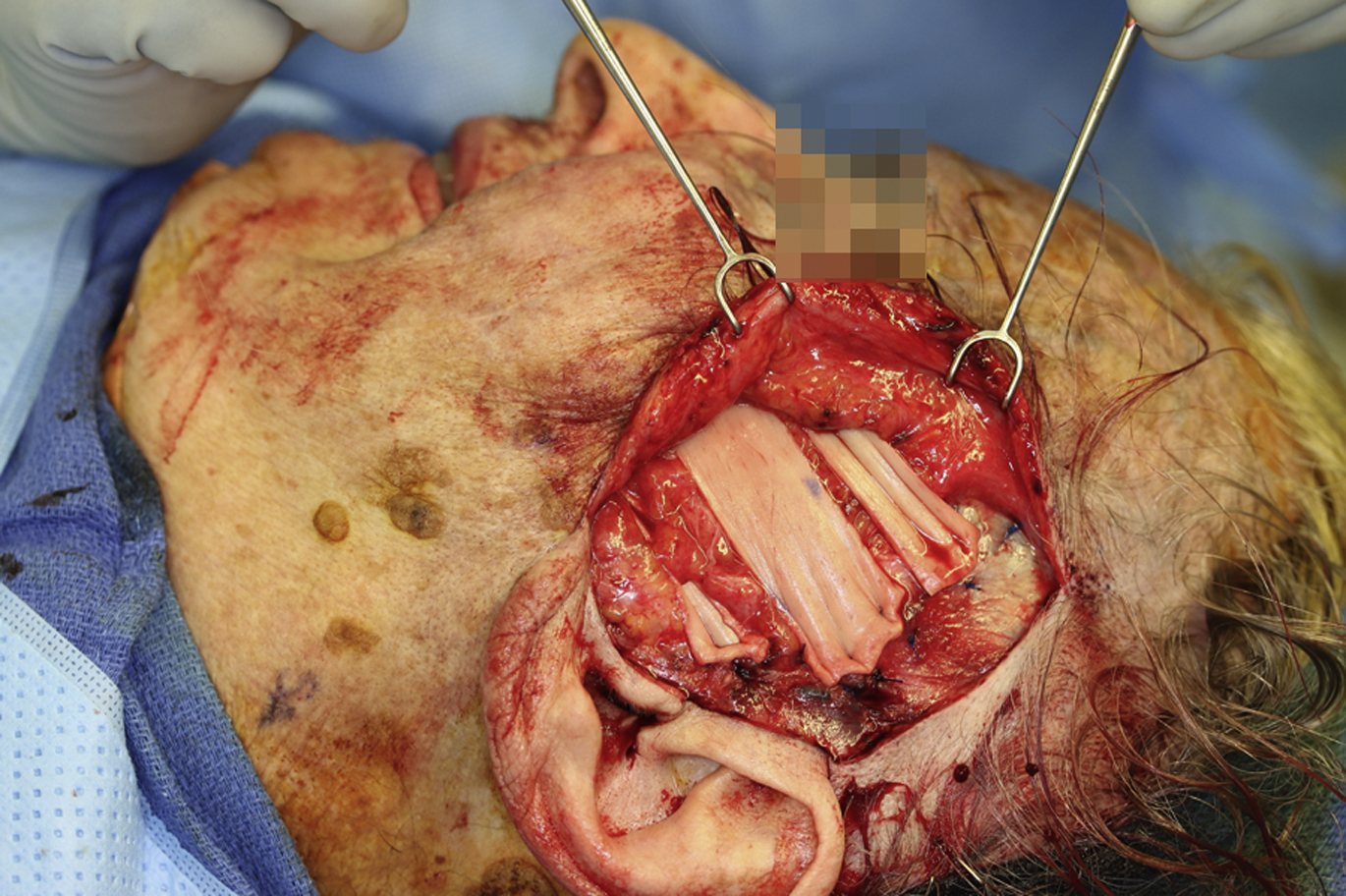
As mentioned previously, in contemporary reconstruction, nerve transfers are increasingly preferred to nerve grafts, because of improved functional recovery associated with higher axonal delivery. Therefore, whether the proximal facial nerve is accessible and given that the distal facial nerve branches are intact and free of tumor, the NTM can be used for subsegmental motor input to either the zygomatic or buccal branches of the facial nerve. The NTM is the largest motor branch of the trigeminal nerve whose number of axon counts match well with the facial nerve. The NTM is reliably found in the subzygomatic triangle, bound by the zygomatic arch ( Fig. 2 ), the temporomandibular joint posteriorly, and the frontal branch of the facial nerve. NTM dissection can be started about 3 cm anterior to the tragus and 1 cm to the zygomatic arch, and was found about 1.5 cm deep to the superficial muscular aponeurotic system (SMAS) in this area.

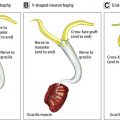
An interesting balancing act is necessary when using combined facial nerve grafts and NTM nerve transfer. Nerve grafts usually offer improved facial tone and limited movement, with some potential synkinesis. The NTM transfer offers greater dynamic commissural excursion, but limited tone. As facial tone is critical for static rest symmetry, and movement is critical for expressivity, an optimal facial reconstructive result would favor the use of both techniques ( Fig. 3 ). Other options for facial symmetry at rest include a hypoglossal nerve transfer. Although there were many possible techniques for achieving the hypoglossal-facial nerve transfer (end-to-end or side-to-end), it often calls for transposition of the main trunk of the facial nerve, which is not usually retained during radical parotidectomy. Use of the hypoglossal nerve in radical parotidectomy reconstruction therefore usually requires an interposition nerve graft. On the other hand, the NTM is in close proximity to the buccal and zygomatic branches, and a tension-free direct end-to-end coaptation is usually possible, even in extensive facial nerve resections. Engagement of smile excursion is also easier using the NTM, as biting down is a more natural action during smiling than pressing the tongue against the teeth or palate. , Using the NTM also has minimal morbidity, because the proximal branch of nerve to masseter remains intact, preserving some degree of masseter bulk and function. Uncommonly, patients may experience ocular discomfort while chewing, or masseter atrophy.

Nerve recovery takes about 6 months but can vary depending on patient age and whether the coaptation was to the zygomatic/buccal branch or a facial nerve trunk. Age greater than 40 and facial nerve trunk anastomoses were associated with longer recovery times. Studies of NTM outcomes show patients were afforded an average of 9 mm of oral commissure excursion and as much as 12.5 mm. ,
Regional Muscle Transfer
The orthodromic temporalis tendon transfer (OTTT) can help immediately restore resting facial symmetry and often commissure excursion and a voluntary, symmetric smile. Performing the temporalis tendon transfer in conjunction with nerve grafting and nerve interposition reduces the duration of loss function while waiting for reinnervation, provides additional movement to reinnervated muscles, and can be used alone when facial nerve recovery is unlikely. An OTTT or lengthening temporalis myoplasty (LTM) may easily be performed in conjunction with an ALT flap to permit immediate restoration of tone, movement, and contour.
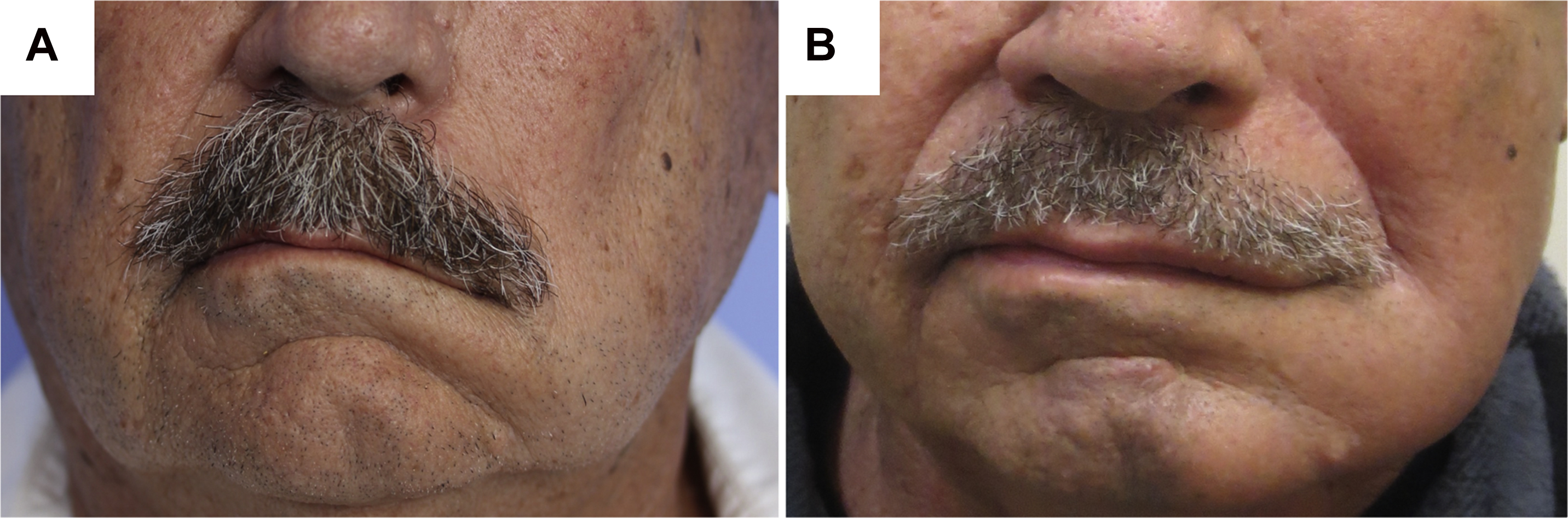
The temporalis muscle is innervated by the anterior and posterior deep temporal nerves, branches of anterior division of the mandibular nerve (CN V3), and these nerves must be spared during ablative surgery. The temporalis tendon insertion to the coronoid process can be approached via an intraoral or transfacial approach. Often it is accessible through the surgical exposure already provided during a radical parotidectomy. The temporalis tendon is mobilized by first dissecting through the buccal space to expose the coronoid process. Using a sagittal or reciprocating saw, the coronoid may be transected and then transposed and attached near the insertion of the zygomaticus muscles at the corner of the lip. The vector of muscle contraction mimics the zygomaticus muscle and helps reestablish the melolabial fold. This can immediately restore resting facial symmetry and dynamic reanimation. House and colleagues (2020) reported that patients undergoing OTTT and LTM were able to attain improved static suspension at rest ( Fig. 4 ) and nearly 5 mm of oral commissure elevation and 3 mm of horizontal excursion. Patients who would later undergo adjuvant radiation therapy to the parotid bed were able to achieve comparable resting symmetry but had worse commissure excursion and an increased risk of postoperative infection compared with their non-irradiated counterparts. In order to optimize a symmetric and spontaneous smile, patients must undergo postoperative muscle retraining and physical therapy. ,
Static Suspension
For patients with significant comorbidities, absence of a functional trigeminal nerve, or inability to tolerate long durations of general anesthesia, performing dynamic procedures may not be appropriate. Instead, performing static suspension to address oral competence, nasal patency, and nasolabial asymmetry provides immediate results with shorter operative times. Static procedures may be performed to complement nerve grafting and other dynamic procedures. Particular to nerve grafting, static procedures provide functional improvements while awaiting reinnervation. Various grafts and implant materials can be used for these static slings including autologous tissue-like tensor fascia lata, allografts, synthetic grafts, or permanent sutures. Fascia lata grafts are preferred over allografts because of lower rates infection and extrusion. Nonvascularized static suspension grafts should be used with particular caution among patients expected to undergo postoperative radiation therapy, as increased risks of infection are expected. Infected grafts are difficult to salvage, may require removal, and may lead to unsightly scarring or failure of suspension. Static slings are used to suspend the alar base, the nasolabial fold, and the oral commissure to the zygomatic arch or the temporalis fascia ( Fig. 5 ). The authors find that it is beneficial to support the lower lip and improve oral competence by suturing fascia lata to the midline lower lip orbicularis muscle and anchoring it to the lateral orbital rim ( Fig. 6 ). The immediate cosmetic outcome may suffer because of the need for mild overcorrection but settles as the suspension material gradually stretches over time.
Related posts:
 Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
 Modified Selective Neurectomy
Modified Selective Neurectomy
 Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
 Dual Nerve Transfer for Facial Reanimation
Dual Nerve Transfer for Facial Reanimation
 Dual Innervation of Free Functional Muscle Flaps in Facial Paralysis
Dual Innervation of Free Functional Muscle Flaps in Facial Paralysis
 Treating Nasal Valve Collapse in Facial Paralysis
Treating Nasal Valve Collapse in Facial Paralysis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


