Total Cranial Vault Remodeling
Akira Yamada
Kenneth E. Salyer
Derek A. Bruce
Frank R. Graewe
DEFINITION/ANATOMY
Premature fusion of the sagittal suture restricts the transverse growth of the skull.
The skull is longer in anteroposterior dimension and narrower in temporal and lateral width.
Frontal and occipital bossing is characteristic, the degree of which depends on the exact location and extent of synostosis (FIG 1).
PATHOGENESIS
Exact cause of primary (isolated) craniosynostosis is unknown.
Sagittal synostosis has an approximately 2% familial or genetic predisposition.
NATURAL HISTORY
Isolated nonsyndromic sagittal synostosis is infrequently associated with abnormal brain development. Intelligence is generally normal, but sagittal synostosis may be associated with subtle psychosocial and learning issues.
PATIENT HISTORY AND PHYSICAL FINDINGS
Physical examination includes assessment of suture ridging in the midline, evidence of other sutural patencies by manual palpation, overall skull and facial configuration, and an age-appropriate neurological examination.
Although papilledema (signs of raised intracranial pressure) is rare in infants with sagittal synostosis, ophthalmologic examination, including visual acuity and the presence of diplopia, can be tested by a pediatric ophthalmologist.
IMAGING
Plain radiographs may be used to document closure of the sagittal suture or to confirm the patency of other sutures.
Adjacent sutures may have compensatory widening due to elevated intracranial pressure.
CT scan of the skull and skull base define brain and skeletal anatomy.
NONOPERATIVE MANAGEMENT
Surgery is routinely advised as soon as the infant is physiologically capable of undergoing surgery.
Nonoperative management is not available for this condition.
SURGICAL MANAGEMENT
Preoperative Planning
Plain radiographs may be used to document closure of the sagittal suture or to confirm the patency of other sutures. Adjacent sutures may have compensatory widening due to elevated intracranial pressure.
CT scan of the skull and skull base define brain and skeletal anatomy.
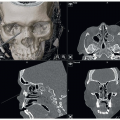
3D reconstruction of the cranium, orbit, and face is useful to use computer-aided design planning, especially for secondary cranial vault reconstruction (FIG 2).
In suspected cases, MRI may be used to rule out the risk of tonsillar herniation, as in Arnold-Chiari malformation.
The cranial vault is removed in three sections. Designing a new bandeau posterior to the coronal suture is the key point of reference for remodeling.
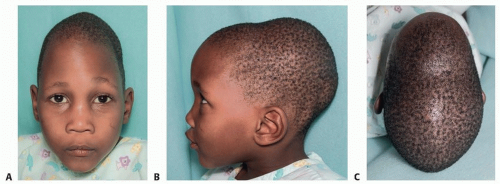
FIG 1 • Preoperative views: frontal (A), left profile (B), and overhead (C).
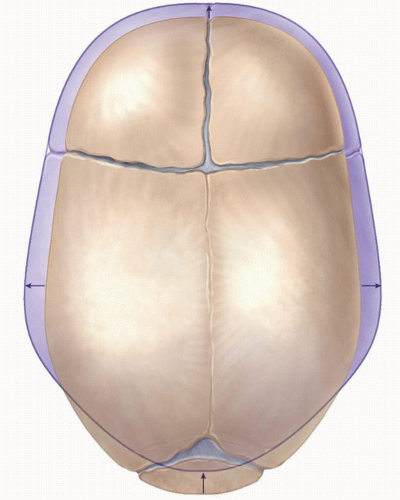
FIG 2 • Preoperative skull shape, in comparison with the goal of surgery (normalization of skull shape), as shown in purple. Goals are to widen at the posterior side, shorten in anteroposterior dimension, smooth the forehead, and make the occipital bone round.
Access to the brain is planned using a bifrontal craniotomy, with expanding and widening of the forehead using the new bandeau and shortening of the anteroposterior dimension of the head.
Positioning
The authors use a supine position for total cranial vault remodeling.
Other centers use a modified prone position for total cranial vault remodeling.
Approach
If the child presents at an age of less than 3 to 5 months, there are three options for treatment:
Endoscopic strip craniotomy with helmet therapy
Extended suture craniotomies with or without dynamic reduction of the abnormally long anteroposterior axis with parietal and occipital extensions
Total cranial vault remodeling1
Simple strip craniotomies with no further remodeling may result in suture refusion with persistence of an abnormally shaped head.
If the child presents at 1 year or older in age, neither simple strip craniotomies nor extended suture craniotomies are appropriate:
Total cranial vault remodeling2 is the first and only choice for treatment.
In this age group, the bone is generally much less malleable than in the child less than 1 year old, and bone remodeling techniques are adapted to the more brittle nature and handling characteristics.
TECHNIQUES
▪ Exposure
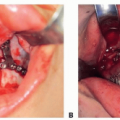
A zigzag skin incision is marked prior to preparation (TECH FIG 1).
The initial incision is made with the Colorado needle and continued laterally on both sides simultaneously.
The scalp is raised above the periosteal, and under the galeal, plane.
The scalp dissection initially proceeds anteriorly first in the same subgaleal/supraperiosteal plane, until 2 cm above the supraorbital rim.
A subperiosteal dissection is then initiated to identify the supraorbital nerves bilaterally, which are released from the bony canal using a small osteotome bilaterally.
Malleable retractors protect the globe.
Further subgaleal/supraperiosteal skin flap dissection is performed in the occipital region.
 TECH FIG 1 • The child is placed in a supine position, and the skin is marked for a zigzag incision.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|