Open Treatment of Mandible Fractures
Joseph Baylan
H. Peter Lorenz
DEFINITION
Mandible fractures are one of the most common facial bone fractures.
Without adequate treatment, fractures of the mandible can lead to malocclusion, condylar resorption, and poor functional and cosmetic outcomes.1
The mandible is a U-shaped bone composed of thick buccal and lingual cortices with a thin medullary canal.
The mandible is divided into paired condyle, coronoid, ramus, angle, body, parasymphysis areas with a single midline symphysis, and tooth-bearing alveolus (FIG 1).
Blood supply to the mandible comes from the inferior alveolar artery and direct muscular attachments.
The inferior alveolar nerve traverses the mandible in the medullary canal, exiting at the mental foramen which is located inferior to the second premolar.
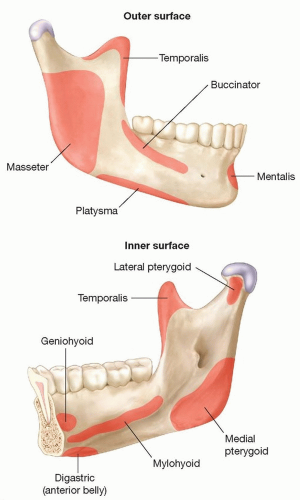
Muscles inserting on the mandible (FIG 2):
Muscles of mastication
Masseter
Temporalis
Medial pterygoid
Lateral pterygoid:
Suprahyoid muscles
Digastric
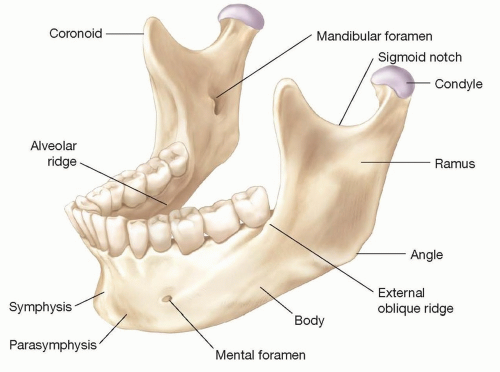
FIG 1 • Bony anatomy of the mandible.
Stylohyoid
Mylohyoid
Geniohyoid
PATHOGENESIS
Two most common causes of mandible fractures are assault and motor vehicle collisions.
Additional causes include gunshot wounds, falls, and sports injuries.
Condylar (36%)
Body (21%)
Angle (20%)
Symphysis (14%)
Alveolar ridge (3%)
Ramus (3%)
Coronoid fractures (2%)
Displacement of fracture segments commonly occurs from differing forces of inserting muscles3:
Muscles of mastication displace posterior segments superiorly.
Suprahyoid muscles displace anterior segment inferiorly.
The lateral pterygoid displaces condylar head medially.
Favorable mandible fractures3:
Unfavorable mandible fractures3:
Horizontal angle fractures that extend posteriorly and downward tend to be displaced by muscles of mastication.
Vertical symphyseal and parasymphyseal fractures are displaced downward by suprahyoid muscles.
High condylar fractures are displaced medially by the lateral pterygoid muscle.
PATIENT HISTORY AND PHYSICAL FINDINGS
Focused history and physical exam:
Mechanism of injury.
Full intraoral and dental examination.
Evaluate for anterior or posterior open bite in centric occlusion.
Evaluate for deviation of the mandible upon opening.
Palpate condyles in preauricular area and external auditory canal during opening to assess translation and tenderness.
Evaluate for mental nerve paresthesias.
Tips.
Use tongue blade intraorally for complete soft tissue evaluation.
Gingival lacerations are typically present at fracture sites.
Ecchymosis on the floor of the mouth is indicative of mandible fracture.
Chin deviation suggests condylar fracture.
Concomitant injury evaluation:
2.6% of patients with facial fractures will have cervical spine injury.3
IMAGING
Panorex plain films may be used to diagnose mandible fractures.
CT imaging is superior to plain films for diagnosing and evaluating mandibular fractures.
NONOPERATIVE MANAGEMENT
The majority of mandible fractures will require operative intervention.
Nondisplaced, stable fractures with normal occlusion can be treated with soft diet and close follow-up.
Greenstick-type fractures or minimally displaced fractures in children with normal occlusion can also be treated nonsurgically.3,4
In the case of edentulous mandibles, minimally displaced fractures can be treated nonoperatively.3
SURGICAL MANAGEMENT
The main goal of operative intervention for mandible fractures is to restore preinjury occlusion and restore mandibular form and function.2
Antibiotics:
All patients with mandible fractures should receive prophylactic antibiotics from the time of injury until the fracture is treated.
This practice has been shown to reduce postoperative infection from 50% to 6%.2
Penicillin-based antibiotic is preferred or clindamycin for patients with penicillin allergy.
Postoperative antibiotics have been shown to have no effect on infection rates.2
Fracture patterns to consider:
Symphysis and parasymphysis: fracture is located in the anterior mandibular portion between the canine teeth.
Body: fracture is located between canine and distal last molar.
Angle or ramus: fracture is located posterior to the second molar and triangle between the horizontal and ascending ramus and often involving the third molar.
Condylar and subcondylar fracture: fracture is located superior to the ramus and is classified according to levels.
Indications for open reduction and internal fixation (ORIF):
Severely displaced fractures
Bilateral fractures
Open fractures
Comminuted fractures
Multiple fracture sites
Panfacial fractures
Infected fractures
Uncooperative patients
Patients with relative contraindication to MMF secondary to medical conditions (seizures, malnutrition, etc.)
Indications for external fixation6:
Bridge until ORIF
Large segmental defect
Severe comminution
Infection present
Indications for removal of the teeth:
Grossly mobile teeth with periapical pathology or advanced periodontal disease
Teeth preventing fracture reduction
Fractured tooth root
Exposed root apices
Preoperative Planning
Nutrition optimization is important for postoperative healing.
For patients with edentulous mandibles, consider the creation of an intraoral prosthesis to help establish maxillarymandibular relation.2,3Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree