Reverse Distraction to Create a Temporomandibular Joint
Joseph Lopez
Anand R. Kumar
DEFINITION
Distraction osteogenesis is a process of slow bone expansion in which new bone forms between an osteotomy gap secondary to tension stresses placed across the bone gap.1
Functional remodeling—the process of functional tissue formation— can be used to create a neocondyle through distraction osteogenesis.
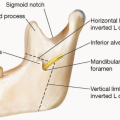
ANATOMY
The mandible is composed of seven zones: symphysis, body, dentoalveolar, angle, ramus, coronoid, and condyle.
The mandible articulates with the squamous portion of the temporal bone at the condyle by forming the temporomandibular joint (TMJ).
The TMJ allows rotational and translational movement of the mandible.
The TMJ joint is surrounded by several muscles:
The masseter muscle, temporalis muscle, medial and lateral pterygoid muscles elevate or protrude the mandible.
The superior portion of lateral pterygoid inserts on the fibrous capsule and meniscus of the TMJ (stabilizes the meniscus during movement of the mandible).
The inferior portion of the lateral pterygoid inserts on the neck of the condyle (helps protrude the mandible when contracting).
The geniohyoid muscle and the anterior belly of the digastric muscle depress and retract the mandible.
All muscles are innervated by cranial verve V.
The TMJ articular surface (articular disc) contains a dense fibrous, connective tissue known as fibrocartilage (unlike other synovial joints, which contain hyaline cartilage).
The central portion of the TMJ articular disc (fibrocartilage) is avascular, whereas the periphery is innervated and receives a tributary of blood vessels. The retrodiskal tissue, which is responsible for the nutrition of the TMJ, are perfused by branches of the maxillary artery (posterior auricular, anterior tympanic, and meningeal medial arteries), drained by the temporomandibular veins, and innervated by the auriculotemporal and posterior auricular nerves.
This fibrocartilage material divides the region of the joint into two spaces:
The upper joint space extends from the glenoid fossa to the articular eminence.
The lower joint space begins above the insertion of the lateral pterygoid and then spreads out over the condyle.
The upper joint space is involved in translational movement of the mandible (arthrodial).
The lower joint space is involved in rotational movement (ginglymus).
PATHOGENESIS
TMJ reconstruction is required in both pediatric and adult populations. The most common conditions that often require TMJ reconstruction include TMJ ankyloses after resection arthoplasty, micrognathia/retrognathia (hemifacial microsomia), and juvenile idiopathic arthritis that can present in both adult and pediatric patient populations.
TMJ ankylosis refers to a pathologic condition in which the mandible is fused to the cranial fossa by bony or fibrotic tissue. TMJ ankylosis can be caused by trauma, infection, congenital deformities, idiopathic factors, or iatrogenic causes.
Micrognathia is a congenital condition involving an abnormally small mandible. It is associated with upper airway obstruction and tends to occur in conjunction with tongue malposition.
Retrognathia is a condition in which there is lack of development of the mandible; more specifically, it refers to the retruded position of the mandible in relationship to the maxilla.
Juvenile idiopathic arthritis (JIA): JIA is the most common rheumatologic disease in children of unclear etiology that can commonly affect the TMJ.
Other common causes of TMJ pathology include degenerative joint disease, traumatic injury, rheumatoid arthritis, and TMJ ablation following tumor resection.
NATURAL HISTORY
Distraction osteogenesis for TMJ reconstruction involves moving a segment of bone, known as the transport disc, slowly away from the host bone into the defect or future TMJ location (FIG 1).
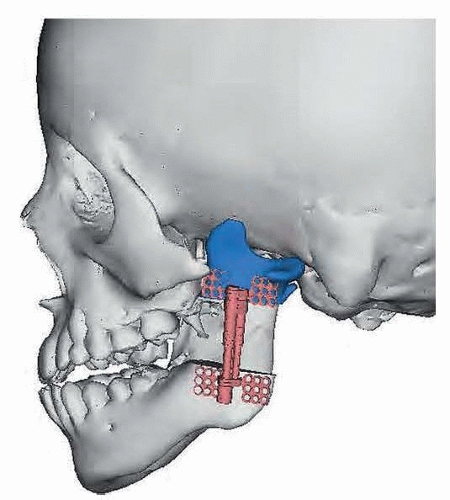
FIG 1 • A digital image demonstrating the transport disc in its new simulated position in the region of the newly generated TMJ joint. Note the vertical vector of distraction and the largest possible piece of bone used as the transport disc.
The transport disc is formed from the vertical ramus remnant or angle of the mandible and is slowly moved into the glenoid fossa or neoglenoid fossa region of the temporal bone.
New bone formation (osteogenesis) occurs at the interface between the transport disc and the host bone. The newly formed bone trailing at the leading edge of the disc forms the new ramus or condylar neck.
Similarly, a fibrocartilagelike structure forms at the disc’s leading edge. This neofibrocartilage cap becomes the new articular surface.
Experimental studies provide support for the remodeling steps described above:
Zhu et al.2 investigated the histomorphologic changes in the newly formed condyle reconstructed by transport distraction osteogenesis in a nonhuman primate model. This study found that “bone regeneration was perfect in the distraction gap between the transport disc and the pre-existing mandible” and the resulting neocondyle was “similar to the original condyle in appearance and structure.”
Similarly, Hikiji et al.3 investigated articular remodeling capacities of distraction osteogenesis for TMJ reconstruction in New Zealand white rabbits and found that after 8 weeks of lengthening, “mature cortical bone” formed between the transport disc and the host bone mandibular segment. Similarly, this experimental study found that a collagenous-like structure formed a cap over the leading edge of the transport segment, suggesting this may “substitute for an articular disc.”
PATIENT HISTORY AND PHYSICAL FINDINGS
Inspection of the head and neck region
Assess soft tissue asymmetry or skeletal deformities.
Assess ear canals and tympanic membrane for primary benign or malignant disease.
Assess dentition for malocclusion, mobility of teeth or prosthetics, or mandibular displacement during teeth contact.
Assess oral mucosa for periodontal disease, mucosal lesions, or swelling.
Assess for overjet, overbite, or open bite.
Neurovascular exam
Cranial nerves 5 and 7 are checked, particularly examining function of the lip depressors (marginal mandibular nerve). This is the most common facial nerve palsy in hemifacial microsomia.
Palpation of the head and neck region
Palpation of the TMJ region to detect crepitus, clicking, or popping
Palpation for swelling or tenderness of the TMJ region
Assess TMJ range of motion (ROM). Normal measurements in adults:
Interincisal opening = 40 to 50 mm
Lateral interincisal movement greater than 10 mm on each side
Any restriction in lateral movement, deviation on mouth opening, or developing of an open bite should be noted.
IMAGING
A panoramic radiograph can identify gross fractures, arthritic changes, bone cysts or tumors, malformation, or bony abnormalities.
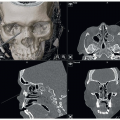
Computed tomography (CT) provides bone pathology information via sectional imaging in both the coronal and sagittal planes (taken in both open and closed joint positions)
CT remains the most frequently used modality to image in 2D and 3D the abnormal bone defect or morphology. The CT can also be used to perform virtual surgical planning (FIG 2).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree