Medial Orbital Wall Fractures
Brad M. Gandolfi
Reena Bakshi
Reza Jarrahy
DEFINITION
Medial orbital wall fractures are traumatic injuries of the orbit that compromise the integrity of the medial orbital wall.
These typically occur at the lamina papyracea, the thin central portion of the medial orbital wall, and may involve herniation of periorbital soft tissues into the adjacent ethmoid sinuses.
ANATOMY
Bony Anatomy
The overall configuration of the bony orbit is pyramidal, with walls that are curvilinear.
The height of the orbit averages 35 mm, with an average width of 40 mm.
The distance from the midpoint of the inferior orbital rim to the orbital apex measures approximately 45 mm.
The medial orbital wall is the thinnest wall of the orbit. It is primarily composed of the lacrimal bone anteriorly and the orbital plate of the ethmoid bone posteriorly.
These structures are closely related to the orbital processes of the frontal, sphenoid, maxillary, and palatine bones.
Ethmoid bone:
The orbital plate of the ethmoid bone accounts for the largest portion of the medial orbit wall. It is also the thinnest portion of bony orbit.
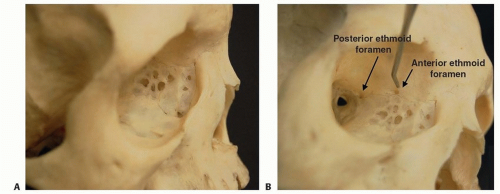
FIG 1 • A. Skull model demonstrating the thin nature of the lamina papyracea and the network of ethmoid air cells lying medial to the orbit. B. The anterior and posterior ethmoid foramen are located on the frontoethmoidal suture.
The thin curved central area of this bone is referred to as the lamina papyracea. Due to its thin nature, most medial orbital wall fractures occur through the lamina papyracea, as opposed to the thicker anterior and posterior portions of the medial orbit.
An extensive labyrinthine network of honeycomblike pneumatized air cells forms the ethmoid sinus medial to the lamina (FIG 1A).
Frontal bone:
The orbital process of the frontal bone articulates with the ethmoid bone in the superior and posterior portion of the bony orbit.
The frontal bone is thicker than the lamina papyracea, providing protection to adjacent intracranial structures.
The roof and medial wall of the orbit meet at the frontoethmoidal suture. The anterior and posterior ethmoidal arteries, branches of the ophthalmic artery, enter the orbit through their respective foramina in the frontoethmoidal suture (FIG 1B).
The anterior ethmoid foramen is located approximately 15 mm posterior to the medial orbital rim and the posterior foramen is located approximately 10 mm further posteriorly.
Disruption of the anterior and/or posterior ethmoid arteries contributes to hemorrhage in the setting of medial orbital wall fractures.
Lacrimal bone:
The lacrimal bone is related to the anterior and inferior aspects of the ethmoid bone.
The central portion of the lacrimal bone is characterized by a depression—the lacrimal fossa—that contains the lacrimal sac. This central recessed portion of the lacrimal bone is surrounded by the anterior and posterior lacrimal crests.
The medial canthal tendon inserts onto the anterior and posterior lacrimal crests.
Sphenoid bone:
The sphenoid bone abuts the posterior edge of the orbital plate of the ethmoid bone.
It delineates the most posterior portion of the medial orbital wall and defines the optic foramen in the orbital apex.
Soft Tissue Anatomy
Knowledge of the soft tissue anatomy of the medial orbit is necessary to safely and effectively manage medial orbital wall fractures without inadvertently injuring surrounding critical structures.
Lacrimal caruncle and plica semilunaris (semilunar fold):
The lacrimal caruncle sits at the medial corner of the eye between the upper and lower eyelids, in close proximity to the medial canthal tendon. It is a fleshy nodule that contains sebaceous and sweat glands that help maintain normal ocular physiology.
It serves as a useful anatomical landmark for surgical approaches to the bony orbit.
The plica semilunaris is a fold of conjunctiva that sits between the caruncle and medial sclera. The plica assists in normal tear function and facilitates movement of the globe (FIG 2A).
Medial canthal tendon:
The medial canthal tendon is associated with the orbicularis oculi muscle and defines the shape and position of the medial poles of the upper and lower eyelids.
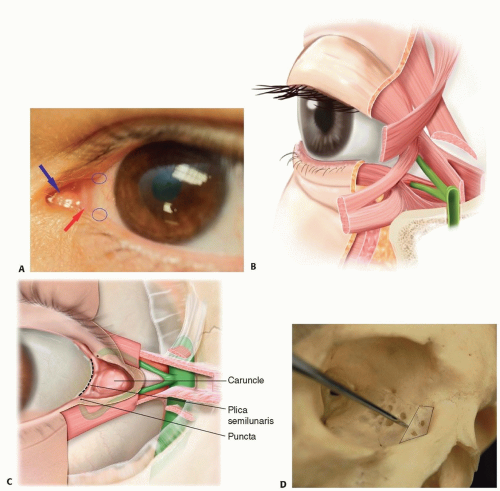
FIG 2 • A. The caruncle (blue arrow) and plica semilunaris (red arrow) help regulate normal ocular physiology and globe movement. The puncta on the upper and lower lids (circled) drain the eye. B. Sagittal section at the level of the attachment of the medial canthal tendon to the lacrimal crest. The medial canthal tendon splits into anterior and posterior components, enveloping the lacrimal sac and canaliculi. C. Relationship between the caruncle (C), puncta (P), the lacrimal apparatus, and the plica semilunaris. The medial canthal tendon has been removed to show the anatomy. The lacrimal fossa (outlined in D) houses the lacrimal sac, which drains through the nasolacrimal duct (E).
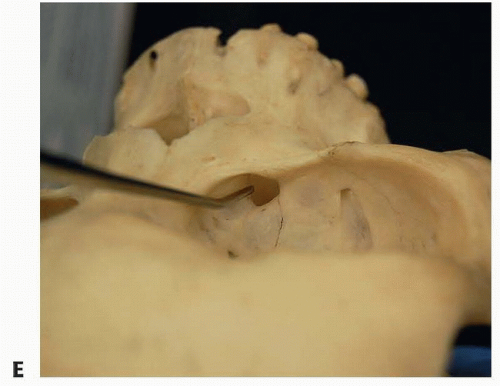
FIG 2 (Continued)
The tendon originates from fascial extensions of the upper and lower tarsal plates and divides into three limbs that insert in a fanlike fashion onto the medial orbital wall.
Disruption of the medial canthal tendon from its bony insertions can have a significant deleterious effect on ocular function and aesthetics (FIG 2B).
Anterior limb:
The anterior limb of the medial canthal tendon inserts onto the anterior lacrimal crest and forms the bulk of the tendon.
The pretarsal, preseptal, and orbital orbicularis fibers insert onto the anterior limb.
Superior limb: The superior limb of the medial canthus extends over the lacrimal sac and covers its anterior and superior portions.
Posterior limb:
The posterior limb of the medial canthal tendon inserts onto the posterior lacrimal crest.
Although not as robust as the anterior limb, its posterior vector is integral in maintaining apposition of the upper and lower lids to the globe.
It is closely related to the Horner muscle, a slip of the lacrimal portion of the orbicularis oculi muscle, which contributes to regulation of normal lacrimal flow.
Lacrimal system:
Puncti: The superior and inferior puncti serve as the primary site of drainage for the eye. They are located approximately 5 to 7 mm lateral to the medial canthal angle (circled in FIG 2A). The upper lid punctum is usually positioned 1 to 2 mm more medial than the lower lid punctum. The majority of tear volume is drained through the lower lid.
Canaliculi: The canaliculi connect the puncti to the lacrimal sac. The ampullae are the vertical components of the canaliculi and are located directly beneath the puncti. The ampullae measure 2 mm in length on average. The canaliculi then turn sharply and extend medially along the border of the eyelid. They merge into a single duct before entering the lacrimal sac (FIG 2C).
Lacrimal sac: The lacrimal sac is located within the lacrimal canal of the lacrimal bone between the anterior and posterior lacrimal crests and the anterior and posterior limbs of the medial canthal tendon (FIG 2C-E). It is partially covered by the superior limb of the medial canthal tendon and extends 5 mm superior to this structure. The sac continues into the nasolacrimal duct at the base of the lacrimal fossa, which continues through an intraosseous tunnel to drain into the nose lateral to the inferior nasal turbinate through the inferior meatus.
Medial rectus muscle: The medial rectus muscle originates at the annular tendon, a fibrous ring surrounding the optic canal at the orbital apex. It inserts onto the medial surface of the globe and is innervated by the inferior division of the oculomotor nerve. Its primary function is to medially adduct the eyeball. Due to its location in the medial orbit, the medical rectus muscle is vulnerable to entrapment in a blow-out fracture through the medial orbital wall.
PATHOGENESIS
Medial orbital fractures typically result from direct blunt trauma to the orbit. Mechanical energy transmitted to the medial orbital wall and/or hydraulic retropulsion of the globe into the orbit can cause structural damage to the medial orbital wall, particularly at the thin lamina papyracea.6
Fractures of the medial orbital wall can play a protective role: absorption of energy by bone limits energy transfer to the orbital soft tissues, decreasing the likelihood of traumatic globe rupture.
NATURAL HISTORY AND PHYSICAL FINDINGS
Symptoms of medial orbital wall fractures include pain with extraocular muscle movement, ecchymoses, and periorbital edema. Physical examination findings include diplopia, enophthalmos, crepitus, visible or palpable medial orbital rim irregularities, and telecanthus.
Cerebrospinal fluid leakage and epistaxis can also be seen in severe orbital injuries that involve adjacent intracranial or nasal structures.
A formal ophthalmological evaluation should be performed to assess baseline ocular function. The ophthalmologist should document a complete examination, including assessment of visual acuity, pupillary reactivity, anterior and posterior ocular chambers, and extraocular muscle function. In the setting of medial rectus muscle entrapment, restriction of extraocular movements may be observed.
IMAGING
Plain film radiography is of limited value in the assessment of medial wall fractures, although disruption of the medial orbit and opacification of the ethmoid sinus can sometimes be detected on x-ray.
Fine-cut axial CT scan with mutiplanar reconstruction has great sensitivity and specificity for identifying medial orbital wall fractures. Two-dimensional axial and coronal views can accurately image the disruption of the medial orbital wall and demonstrate herniation of periorbital soft tissues into the ethmoid sinuses (FIG 3A,B).
Three-dimensional (3D) reconstructions of orbital CT scans are generally not helpful in diagnosing medial orbital wall fractures. The algorithms used by most 3D imaging software programs currently do not provide adequately detailed renderings of the surface anatomy of the thin curved medial orbital wall7 (FIG 3C,D).
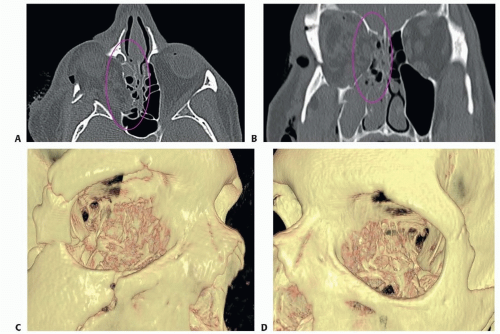 FIG 3 • Axial (A) and coronal (B) computed tomography (CT) imaging of the orbit demonstrating fracture of the (right) medial orbital wall with herniation of periorbital soft tissues into the ethmoid sinus (circled). C,D. 3D rendering of the same injury does not provide a detailed anatomic picture.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|