Segmental Le Fort I Advancement: Two and Three Piece
Leo J. Urbinelli
Jeffrey A. Hammoudeh
DEFINITION
Le Fort I osteotomies (single or multipieced) are performed to reposition the teeth-bearing segment(s) of the maxilla and to surgically correct skeletal malocclusion, dentofacial asymmetries, and midfacial deficiencies or excess.
Segmentation as a multipiece Le Fort I osteotomy is frequently used to modify the transverse dimension of the maxilla to provide a more optimal occlusion between the maxillary and mandibular teeth.
Segmentation is more commonly performed when the presurgical orthodontia is suboptimally leveled, aligned, and coordinated, which is more common in the cleft palate patient.
Skeletal malocclusion is best defined by Dr. Edward Angle’s classification (FIG 1) to assess dentofacial deformities that may require orthognathic surgery or in particular a Le Fort I maxillary advancement.
Class I occlusion is present when the normal relationship of the maxillary to mandibular teeth exists: the mesiobuccal cusp of the maxillary first molar intercuspates within the buccal groove of the mandibular first molar.
In class II malocclusion, the mesiobuccal cusp of the maxillary first molar sits too far anterior and does not seat into the mandibular buccal groove of the first molar, as in the case of mandibular retrognathia.
In class III malocclusion, the mesiobuccal cusp of the maxillary first molar lies posterior to the mandibular first molar’s buccal groove as is seen in mandibular prognathism.
Le Fort I advancement surgery requires the surgeon to understand facial aesthetics, dentofacial relationships, and cephalometric norms in order to accomplish a suitable and stable surgical outcome.
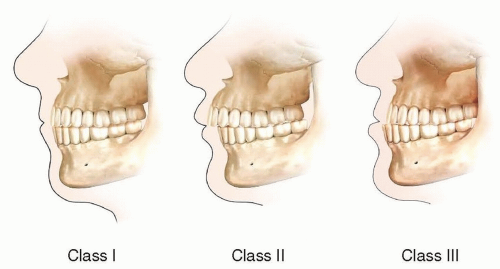
FIG 1 • Angle classification of occlusion.
Cephalometric norms have traditionally been regarded standard in the workup of orthognathic cases and are important from an educational, academic, and historical standpoint.
However, the limitations of cephalometric two-dimensional analysis have led to three-dimensional (3D) computed tomography scanning for virtual surgical planning (VSP).
3D VSP is our recommendation for complex orthognathic surgery.
Two-piece segmental Le Fort I maxillary advancement surgery is indicated when maxillary advancement alone does not correct the transverse discrepancy.
In the noncleft patient, the traditional segmentation of the maxilla is between the two maxillary incisors in a midsagittal osteotomy from the anterior nasal to the posterior nasal spine.
In the cleft patient who has undergone alveolar cleft repair, it is reasonable to consider the segmentation at the alveolar cleft site to mitigate vascular compromise of the segments.
Three-piece segmental Le Fort I maxillary advancement surgery is often indicated in the cleft lip and palate and/or syndromic craniofacial patient, when it is determined from physical exam that the patient has midfacial hypoplasia in the anteroposterior dimension and/or class III malocclusion in the setting of an arch that has suboptimal leveling, aligning, and coordination.
This is exemplified by physical examination, dental model analysis, cephalometric evidence, an acute sella to nasion to A-point angle (SNA angle less than 79 degrees), and VSP analysis (FIG 2).
ANATOMY
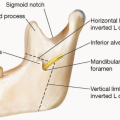
Le Fort I osteotomy is defined by sectioning of the bony maxilla above the apices of the teeth but below the level of the nasal bones, through the nasal septum, and completing the disjunction at the pterygomaxillary junction.
Segmentation of the Le Fort I maxillary segment is done by sectioning the maxilla between the tooth roots to allow expansion or reduction in the transverse plane, often completed after down-fracture of the tooth-bearing maxillary segment.
Segmentation for a two-piece Le Fort is routinely between the maxillary central incisors in a midsagittal osteotomy (FIG 3).
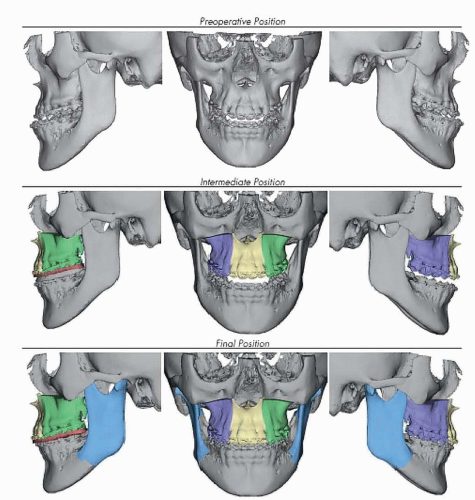
FIG 2 • Virtual surgical plan of three-piece Le Fort I osteotomy.
In the cleft patient who has undergone alveolar cleft repair, if the alveolar cleft repair bone quality/take is less than optimal, it is reasonable to cut at the alveolar cleft site and extend the segmentation to the midsagittal osteotomy.
This technique minimizes the potential vascular risks to the anterior maxillary segment.
Blood supply to the maxilla is rich and redundant in the noncleft patient.
After sectioning of the Le Fort I osteotomy, the blood supply depends on branches of ascending pharyngeal and ascending palatine arteries.
Blood supply to the maxilla in the cleft lip/palate and syndromic craniofacial patient is less abundant and predictable due to potential previous surgical interventions, but maxillary segmentation can be done safely when risk mitigation techniques are used.
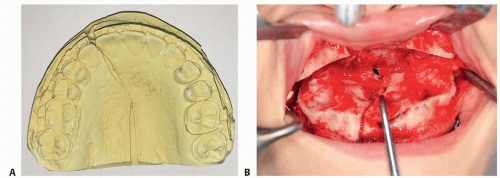
FIG 3 • A. Two-piece Le Fort I segmentation planned using the stone model. B. Intraoperative view after Le Fort I osteotomy, down-fracture, and twopiece segmentation.
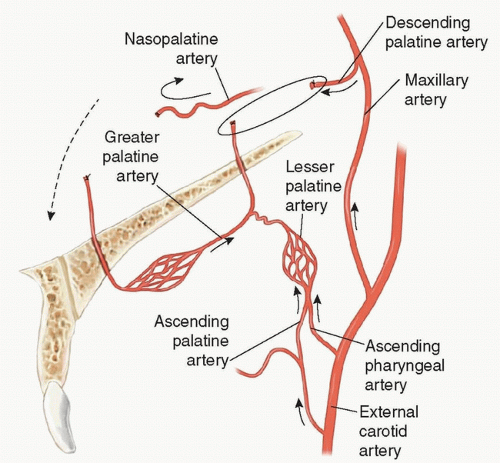
FIG 4 • Palatine arteries after down-fracture in Le Fort I osteotomy.
These techniques include using a high-cuffed gingival incision, minimizing the dissection to what is needed, minimizing the segmentation to a two-piece maxilla if feasible, and keeping the total maxillary advancement to less than 10 mm.
Potential maxillary vascular compromise in a cleft lip/palate patient undergoing a three-piece Le Fort I osteotomy must be discussed with the family and patient preoperatively as this multisegmentation may predispose to a loss of teeth, bone, or even the entire premaxillary segment.
These risks cannot be eliminated, but they can be mitigated using the techniques described above. A threepiece Le Fort segmentation can be performed reliably with stable and predictable results by experienced clinicians.
PATHOGENESIS
Developmental skeletal dysplasia, in particular midfacial hypoplasia and dental class III malocclusion, is a multifactorial skeletal deformity of the face.
Factors contributing to this deformity are genetic, environmental, idiopathic and potentially iatrogenic.
This deformity can be found in cleft, noncleft/nonsyndromic, and syndromic craniofacial patients.
Cleft palate repair and healing have been associated with a higher incidence of midfacial hypoplasia, transverse maxillary discrepancy, and overall malformation of the facial skeleton and dental malocclusion.
Midfacial hypoplasia requiring a Le Fort I advancement is seen in up to 25% of complete cleft lip and palate patients.2
NATURAL HISTORY
Children with orofacial clefts may or may not have normal occlusal relationships in early development; however, as they skeletally develop, maxillary growth often lags behind mandibular growth giving a concave midfacial appearance and class III malocclusion.
With small disturbances in occlusion, orthodontics and headgear can be used to distract the maxilla in reference to the mandible.
However, the natural history of many orofacial cleft patients is that a larger midfacial discrepancy (4-15 mm) of a negative overjet exists, requiring surgical intervention to advance the maxilla in relation to the lower jaw as well as surgically correct transverse discrepancies.
With anterior maxillary advancement of less than 10 mm, the prognosis for low relapse rates and long-standing, stable results can be accomplished with a segmented Le Fort I advancement.
Maxillary transverse expansion is associated with a higher risk of relapse in both noncleft and cleft patients.
The cleft patient transverse relapse risk is higher and is correlated with the history of previous palatal operations, fistula repairs, pharyngoplasty/pharyngeal flaps, sequences/syndromes, and operative technique (fixation technique as well as the overall movement metrics).
We recommend minimizing the segmentation, using rigid fixation and postoperative splint retention with a palatal bar. In some circumstances where fixation is suboptimal, a period of closed reduction is indicated.
PATIENT HISTORY AND PHYSICAL FINDINGS
History should include inquiry into the past medical and dental history, documenting the extent and progress of presurgical orthodontia.
The clinician should note any pain on jaw opening and closing or difficulty eating, speaking, or closing the mouth without strain of the chin. One should also elicit history of prior airway comorbidities, sleep disturbances (obstructive sleep apnea, enlarged turbinates), or prior surgery (palatal, speech or velopharyngeal surgery, prior jaw or nasal surgery).
Additionally, one should ascertain if the patient has completed skeletal growth (continued height, foot, and hand growth), as Le Fort I advancement surgery is most stable and indicated when skeletal maturity is reached.
History of orthodontic treatment (duration, modalities) should be assessed.
Physical examination should include an overall assessment of facial balance and proportions including photo documentation of the frontal, lateral, and oblique face in the repose and in full animation; this should include a focused intraoral exam.
This intraoral exam is imperative to assess overall dental health, missing/diseased teeth, previous palatal surgery, or scarring over the buccal/gingival mucosa.
Intraoral pictures should be obtained of midline occlusal as well as bilateral canine to mandibular molar relationships.
Intraoral exam should include inspection of orthodontia (wires, brackets, hooks, etc.) and clearly identify the dental malocclusion, skeletal dysplasia, and if any maxillomandibular cant exists.
Bimanual palpation of the temporomandibular joint on opening and closing of jaws for preoperative assessment of this complex joint is crucial.
Palatal and oronasal fistulae should be noted. The pharynx should be examined as well as a detailed intranasal exam performed to check for any septal deviation, perforations, or enlarged turbinates.
One of the most effective orthognathic surgical options in addressing midfacial hypoplasia with class III malocclusion is to combine a Le Fort III osteotomy in conjunction with a multiple-piece Le Fort I osteotomy.
This can make a profound change and correct a midface global hypoplasia in conjunction with severe dental malocclusion (FIG 5).
IMAGING AND OTHER DIAGNOSTIC STUDIES
Traditionally, posteroanterior and lateral cephalograms as well as a panoramic x-ray are obtained (FIG 6).
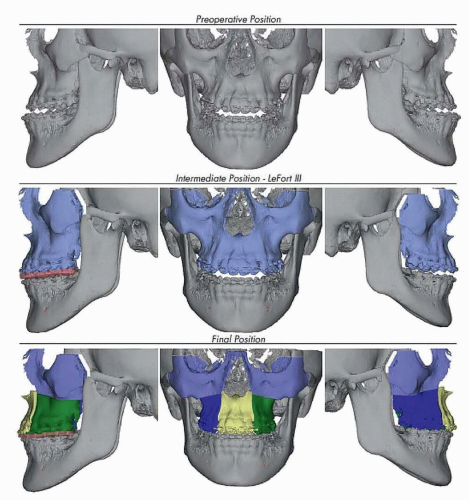
FIG 5 • Virtual surgical plan of combined Le Fort III osteotomy and advancement with three-piece Le Fort I segmentation.
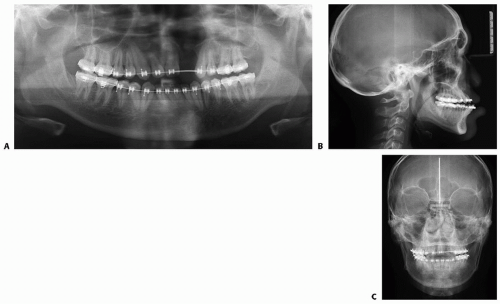
FIG 6 • Panorex (A) and posteroanterior (B) and lateral (C) cephalograms.
Periapical views around missing bone along the alveolus may allow the surgeon to assess if simultaneous bone grafting is needed at time of Le Fort I advancement.
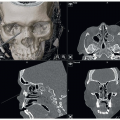
Craniofacial CT scanning has become the mainstay in complex orthognathic surgery and is a requisite for 3D VSP, model, and splint fabrication.
To facilitate the VSP, the preoperative occlusion must be obtained via dental stone models with bite registrations, or a digital dental scan of the teeth can be performed, which is then incorporated into the craniofacial CT for the VSP.
3D tissue rendering can also be used by overlapping the soft tissue window on top of the bony images.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree