There is no universally accepted treatment regimen and no evidence-based literature to guide management of hypertrophic scars. This article summarizes the existing literature regarding topical treatments such as silicone gel sheeting and ointment, onion extract, vitamin E, pressure garment therapy, massage therapy, and topical imiquimod 5% cream in the management of hypertrophic scars.
- •
There is no single, optimal topical modality that can eliminate or prevent hypertrophic scars.
- •
Silicone gel sheeting (SGS) remains the most accepted modality in the treatment and prevention of hypertrophic scar.
- •
Onion extract and vitamin E have not been shown to consistently improve scar appearance as single agents.
- •
Topical imiquimod 5% cream in a small study was shown to improve scarring.
- •
Pressure therapy is described predominantly for management of postburn scars.
- •
Massage therapy is a common modality in the management of scarring in patients with burns, but scientific evidence for its efficacy is limited.
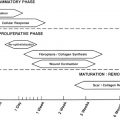
Any cutaneous injury, including surgical incisions, that extends into the dermis will always heal with a scar. The wound healing process is a complex hierarchy of events centered on inflammation, cell proliferation, and remodeling. Cutaneous wounds occasionally heal with scarring that is in excess of what is considered to be a normal physiologic scar. This exuberant scarring results in hypertrophic scars and keloids. Both types of scars are raised, initially pink to purple lesions that are often painful or pruritic. Clinically, hypertrophic scars are limited to the area of original injury with a tendency toward gradual resolution in time. Keloids extend beyond the original wound margin and seldom resolve spontaneously.
Hypertrophic scars are caused by a variety of factors including mechanical forces on the healing wound (excess tension at wound edge, improper suture placement), poor wound healing, bleeding, or infections. Therapeutic modalities for the prevention and management of scars have been postulated to act by correction of abnormal collagen metabolism, alteration of the immune/inflammatory response, or manipulation of the mechanical properties of wound repair. This article focuses on topical treatments such as SGS and ointment, onion extract, vitamin E, pressure garment therapy, massage therapy, and topical imiquimod 5% cream in the management of hypertrophic scars.
SGS
Silicone polymers are inert, mixed inorganic-organic polymers with a wide array of forms and applications. Polydimethylsiloxane is the most widely used silicon polymer, including in medical products such as SGS. The mechanism of action of SGS is uncertain, but has been postulated to be caused by hydration and occlusion, increased oxygen tension, and the production of a local static field, all of which result in improved remodeling of the scar. The beneficial effects of SGS were first shown in 1983 by Perkins and colleagues in patients with burn scars and contractures. In a controlled study comparing SGS and nonsilicone gel dressing, de Oliveira and colleagues reported improvement in size and induration of hypertrophic scars and keloids in both groups compared with control, but there was no significant difference in results between SGS and nonsilicone gel dressing groups. This finding further suggests that the mechanism of SGS is related to hydration and occlusion.
Several studies have been reported to show clinical efficacy in the treatment of hypertrophic scars with SGS. Ahn and colleagues reported clinical and elastometric improvement of hypertrophic burn scars treated with SGS for 8 weeks compared with untreated scars. The improvement in scar volume lasted up to 6 months. Momeni and colleagues performed a randomized, double-blind, placebo-controlled split-scar trial involving 38 people with hypertrophic burn scars. Using the modified Vancouver Scar Scale, he showed an improvement in pigmentation, vascularity, pliability, and pruritus of treated scars after 4 months of treatment. A prospective controlled study investigating 42 patients with 47 hypertrophic scars comparing 2 types of SGS with no treatment showed improvement in scar color and induration in the treatment group. However, in the study by de Oliveira and colleagues, who compared SGS with nonsilicone gel sheets, there was no difference in scar size or induration between the 2 groups.
The usefulness of SGS in the prevention of scar formation has also been shown. In a prospective study of 20 women with bilateral reduction mammaplasties, patients were instructed to use SGS to 1 breast for 12 hours each day for 2 months. At 2 months, 60% of the nontreated scars were hypertrophic and only 25% of the treated scars were hypertrophic ( P <.05). Conversely, in another split-scar study of 155 women who underwent reduction mammaplasties, comparing SGS and nonocclusive Micropore (3M, Ad Leiden, The Netherlands), there were no difference in the occurrence of hypertrophic scarring between the SGS-treated and untreated portions of the scars. Gold and colleagues treated 96 patients who had undergone skin surgery with routine postoperative care or topical SGS for 48 hours after surgery. They showed that patients with a history of abnormal scarring had a lower rate of developing hypertrophic or keloid scar when treated with SGS compared with routine postoperative care (39% vs 71%). In the patients who subsequently underwent scar revision, 36% of patients treated with SGS developed recurrent abnormal scar versus 83% (10 patients) within the routine wound care group. Most recently, in a case series of 7 patients, a liquid silicone gel applied twice a day for 3 months to one-half of a new surgical scar was reported to show noticeable improvement in scar appearance.
In a meta-analysis of SGS for the prevention or treatment of hypertrophic or keloid scars, SGS was found to reduce the incidence of hypertrophic scarring for individuals prone to scarring (relative risk [RR], 0.46; 95% confidence interval [CI], 0.21–0.98). Overall, a significant reduction in scar thickness (RR, −1.99; 95% CI, −2.13 to −1.85) and color amelioration (RR, 3.05; 95% CI, 1.57–5.96) was observed. However, the studies reviewed were deemed highly susceptible to bias. In 2002, an international advisory panel after reviewing more than 300 published articles recommended SGS as a primary option in the management of hypertrophic or keloid scars.
Based on our review of current published studies on SGS, this modality should be considered in the treatment and prevention of hypertrophic scars. The authors typically advise the patients with the earliest signs of hypertrophic scaring to use over-the-counter (OTC) SGS sheets daily for up to 2 months as tolerated. Based on our experience, there are minimal risks, and there is improvement in scar thickness.
Vitamin E
Vitamin E is a family of essential micronutrients composed of lipid-soluble tocopherols and tocotrienols with strong antioxidant activity. The proposed mechanism of action of vitamin E in modulation of wound healing and scar formation is inhibition of collagen synthesis, and it reduces both fibroblast proliferation and inflammation. It is used by the general population to treat wounds, burns, and surgical incisions, with the belief that it improves the cosmetic outcome of scars. In a double-blinded, controlled study, 15 patients who had undergone skin cancer removal surgery applied Aquaphor with and without vitamin E to their wounds twice daily for 4 weeks. In 90% of the cases in this study, topical vitamin E either had no effect on, or worsened, the cosmetic appearance of scars. Of the patients studied, 33% developed a contact dermatitis to the vitamin E. A study of 159 operative procedures for postburn contractures treated postoperatively for 4 months with topical vitamin E showed no beneficial effect in cosmetic appearance or reducing scar formation, but was associated with increased adverse reactions. In a recent prospective, randomized, double-blinded study on 122 patients with surgical scars less than 2 weeks old, topical tocotrienol twice a day for 6 weeks showed no significant difference in treatment and placebo groups using the Patient and Observer Scar Assessment Scale (POSAS), a photographic scar assessment by 2 independent assessors using a visual analogue scale and laser Doppler imaging (LDI).
A limited number of studies have shown a potential beneficial effect with vitamin E. Eight adult patients with hypertrophic scars and keloids were treated with SGS with and without vitamin E. Using a visual analogue scale, a 50% scar improvement was noted in 95% of patients treated with combined vitamin E and SGS compared with 75% of patients treated with SGS alone; the improvement was statistically significant. In another randomized controlled study a combination lotion of silicone and vitamin E showed significant improvement in scar induration, pigmentation, and erythema compared with placebo. Given that the aforementioned 2 studies used a combination of silicone and vitamin E in the active arm, it is unclear whether the silicone or vitamin E component played a larger role in the improvements seen. In a recent study on children with perioperative topical vitamin E on the incision site showed that 96% of patients treated with topical vitamin E reported good cosmetic results compared with 78% of patients treated with emollients.
Based on our review of current published studies on topical vitamin E, and the lack of scientific evidence, we do not recommend the routine use of topical vitamin E for management and prevention of postsurgical scars. In addition, contact allergy is a potential risk with the use of this agent.
Vitamin E
Vitamin E is a family of essential micronutrients composed of lipid-soluble tocopherols and tocotrienols with strong antioxidant activity. The proposed mechanism of action of vitamin E in modulation of wound healing and scar formation is inhibition of collagen synthesis, and it reduces both fibroblast proliferation and inflammation. It is used by the general population to treat wounds, burns, and surgical incisions, with the belief that it improves the cosmetic outcome of scars. In a double-blinded, controlled study, 15 patients who had undergone skin cancer removal surgery applied Aquaphor with and without vitamin E to their wounds twice daily for 4 weeks. In 90% of the cases in this study, topical vitamin E either had no effect on, or worsened, the cosmetic appearance of scars. Of the patients studied, 33% developed a contact dermatitis to the vitamin E. A study of 159 operative procedures for postburn contractures treated postoperatively for 4 months with topical vitamin E showed no beneficial effect in cosmetic appearance or reducing scar formation, but was associated with increased adverse reactions. In a recent prospective, randomized, double-blinded study on 122 patients with surgical scars less than 2 weeks old, topical tocotrienol twice a day for 6 weeks showed no significant difference in treatment and placebo groups using the Patient and Observer Scar Assessment Scale (POSAS), a photographic scar assessment by 2 independent assessors using a visual analogue scale and laser Doppler imaging (LDI).
A limited number of studies have shown a potential beneficial effect with vitamin E. Eight adult patients with hypertrophic scars and keloids were treated with SGS with and without vitamin E. Using a visual analogue scale, a 50% scar improvement was noted in 95% of patients treated with combined vitamin E and SGS compared with 75% of patients treated with SGS alone; the improvement was statistically significant. In another randomized controlled study a combination lotion of silicone and vitamin E showed significant improvement in scar induration, pigmentation, and erythema compared with placebo. Given that the aforementioned 2 studies used a combination of silicone and vitamin E in the active arm, it is unclear whether the silicone or vitamin E component played a larger role in the improvements seen. In a recent study on children with perioperative topical vitamin E on the incision site showed that 96% of patients treated with topical vitamin E reported good cosmetic results compared with 78% of patients treated with emollients.
Based on our review of current published studies on topical vitamin E, and the lack of scientific evidence, we do not recommend the routine use of topical vitamin E for management and prevention of postsurgical scars. In addition, contact allergy is a potential risk with the use of this agent.
Onion extract
Allium cepa (onion extract) is a common ingredient in several commonly used OTC scar therapy agents. A cepa has been found to contain both antibacterial and fibrinolytic activity. Mederma (Contractubex, Merz, Frankfurt, Germany), is a topical gel containing 10% aqueous A cepa as the active ingredient. The other components of Contractubex gel are 50 IU heparin per gram of gel and 1% allantoin. A few studies have examined the potential effects of onion extract in treatment of surgical scars. In an open trial of Contractubex gel in patients with surgical wounds after thoracic surgery, Willitel and colleagues reported a reduced scar width and reduced frequent of hypertrophic and keloidal scars in the treatment group. In a separate study, Ho and colleagues evaluated the efficacy of Contractubex gel in the prevention of scarring after laser removal of tattoos in 120 Chinese patients. They reported a lower rate of scarring in the treatment group (11.5% in the treatment group vs 23.5% in the control group). Koc and colleagues studied the combination of intralesional triamcinolone and topical onion extract gel versus intralesional triamcinolone alone in 27 patients with keloid or hypertrophic scars of 1 year or more in duration. They reported that intralesional triamcinolone with topical onion extract was more effective than intralesional triamcinolone alone in pain sensitiveness, itching, and elevation but not in erythema and induration. This study was not blinded and lacked a placebo-controlled arm. Campanati and colleagues studied the effect of topical onion extract gel in 30 patients with hypertrophic or keloid scars using intravital videocapillaroscopy, and reported significant reduction in neoangiogenetic features, shown by an improvement in erythema and all videocapillaroscopic markers of neoangiogenesis. In another blinded, placebo-controlled study, 60 postshave excision sites were treated with an onion extract gel. Onion extract treatment resulted in improvements in scar redness, pliability, texture, and the global appearance. Perez and colleagues reported that significant improvements were obtained with onion extract in volume, length, width, and induration of hypertrophic and keloidal scars with a combination of onion extract gel and 0.5% hydrocortisone.
Jackson and colleagues studied 17 patients with surgical scars resulting from Mohs surgery who were treated with topical onion extract or petrolatum-based ointment from suture removal for 1 month. They reported no statistically significant difference between pretreatment and posttreatment evaluations of scar erythema and pruritus in patients using topical onion extract gel. Instead, a statistically significant reduction in scar erythema was found in patients using a petrolatum-based ointment. A subsequent prospective randomized, double-blinded, split-scar study comparing topical onion extract gel and petrolatum-based ointment in 24 patients with new surgical wounds after Mohs or excisional surgery also found no significant difference in scar erythema, hypertrophy, or overall cosmetic appearance.
Review of the published studies on the usefulness of onion extract shows weak to no significant improvement for prevention and improvement in hypertrophic scarring. In addition, many of the reported studies lack a proper control arm. The authors do not routinely recommend the use of these agents in their clinical practice.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


