Keloids result from an abnormal wound-healing process in which the normal regulatory pathways during tissue regeneration and scar remodeling are disrupted. While the pathogenesis of keloids continues to be investigated, numerous treatment options exist. Although prevention of keloid formation is the best management, early recognition of keloid formation is integral in treatment and prevention of recurrence. Surgical resection with adjuvant silicone gel sheeting or triamcinolone injection is common, but can still result in recurrence. New treatments include chemotherapeutics such as 5-fluorouracil, bleomycin, and mitomycin C. Although further clinical investigation is required for newer treatments, initial results are promising.
- •
Keloids can be difficult to differentiate clinically from hypertrophic scars; however, there are distinguishing characteristics of each
- •
The pathophysiology of keloids continues to require ongoing research
- •
Surgical excision followed by intralesional steroid injection is considered a first line treatment
- •
Silastic gel sheeting can improve keloid appearance when used appropriately
- •
Radiation can be a safe and effective means of keloid treatment with the appropriate precautions
- •
Topical application of chemotherapy medication is a reasonable alternative in patients with keloid recurrence after surgical excision and steroid treatment
Pathophysiology and histology
Wound healing is tightly regulated, and errors in the process can manifest anywhere along the pathologic spectrum from chronic wounds to the aggressive scar formation seen in keloids, the latter being the topic of interest here. On the subject of keloids, hypertrophic scars must also be mentioned because the two are often, incorrectly, used interchangeably. This distinction must be made, as the appropriate application of current and future interventions mandates understanding the clinical, histologic, and biochemical pathology of keloids.
Keloids can occur immediately after trauma, or grow months after a mature, stable scar has formed. This trauma can range from vaccination needle sticks, lacerations, bug bites, and burns, to dermatologic conditions such as acne or folliculitis. In all cases, the end result is skin inflammation. Hypertrophic scars follow the pattern of evolution, stabilization, and involution within the boundaries of the original wound. By contrast, keloids continue to proliferate, resulting in a raised, erythematous scar with a wide variability of height progression and scar distribution. As such, keloids will grow outside the boundaries of the original scar. Although keloids can reach a quiescent phase, very rarely do they regress. Lee and colleagues found that symptomatically, 46% of patients noted keloid-associated pain and 86% noted pruritis.
Keloids affect darker-skinned individuals approximately 15 times more than Caucasians, suggesting a genetic factor. Keloids affect roughly 15% to 20% of the African American and Hispanic populations. Keloids typically occur during and after puberty, between the ages of 10 and 30 years. Although there is no gender predilection, keloids can regress during menopause or worsen during pregnancy.
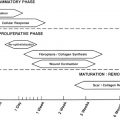
The pathogenesis of keloids continues to undergo investigation, and understanding this process requires knowledge of the normal wound-healing process. Normal wound healing occurs in 3 stages : the inflammatory phase, the proliferative/granulation phase, and the maturation/remodeling phase. The inflammatory phase begins immediately after the injury. Hemostatic mechanisms of platelet degranulation and activation of complement and clotting cascades occur quickly. Cytokines and growth factors such as transforming growth factor β (TGF-β), platelet derived growth factor (PDGF), and epidermal growth factor (EGF) are released through platelet degranulation and from the surrounding tissue. These cytokines and growth factors induce the influx of neutrophils, macrophages, mast cells, and epithelial cells. After the first 24 to 48 hours, the inflammation is perpetuated by mast cells and neutrophils and can last for anywhere from 3 to 8 days. Macrophages aid in wound debridement as fibroblasts and smooth muscle cells migrate into the wound. Prolongation of this phase occurs in cases of large wounds or in the presence of infection, and results in greater exposure to fibrogenic cytokines.
During the proliferative phase, at approximately 3 to 6 weeks, fibroblasts deposit type III collagen and synthesize granulation tissue, composed of procollagen, elastin, proteoglycans, and hyaluronic acid. This scaffold allows the ingrowth of vasculature, and with wound contracture and closure facilitated by myofibroblasts, allows the wound to undergo continued remodeling in the final phase of wound healing.
The maturation/remodeling phase can take from several months to more than a year. During this phase, the type III collagen is replaced by stronger type I collagen fibers. Proteoglycans are synthesized, and fibrin and fibronectin are degraded. In addition, the extracellular matrix produced by fibroblasts undergoes simultaneous degradation by mostly serine proteases (ie, tissue plasminogen activator and urokinase plasminogen activator) and matrix metalloproteinases (MMPs). Collagen fibers are rearranged, cross-linked, and aligned along tension lines. The tensile strength of the scar improves, but at best achieves only 80% the tensile strength of normal skin.
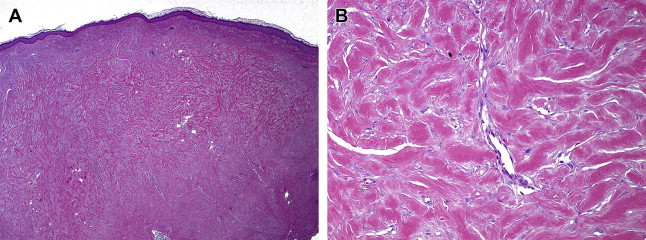
Histologically, keloids invade the normal surrounding dermis, a distinct difference from hypertrophic scars, which stay within the confines of the wound borders. In keloids, collagen fibers are larger, thicker, wavier, and oriented haphazardly. Collagen fibers in hypertrophic scars and normal scars are oriented parallel to the epidermal surface. The collagen fibers in keloids are arranged into thick collagen bundles that are packed tightly together within the dermis, where there is a lack of sebaceous glands and rete ridges. These collagen bundles are also found to lack the presence of myofibroblasts. Hypertrophic scars form fibrous nodules composed of fibroblasts, mostly type III collagen fibers, and vessels. By contrast, keloid scars form nodules with reduced vascularity and a hypocellular appearance ( Fig. 1 ). This acellular core within keloids is characterized by thick bundles of type I and type III collagen fibers interspersed with fibroblasts (see Fig. 1 B).
Related posts:
 Use of Makeup, Hairstyles, Glasses, and Prosthetics as Adjuncts to Scar Camouflage
Use of Makeup, Hairstyles, Glasses, and Prosthetics as Adjuncts to Scar Camouflage
 Use of Hair Grafting in Scar Camouflage
Use of Hair Grafting in Scar Camouflage
 Scars: Clinical Evidence Base and Patient Impact
Skin: Histology and Physiology of Wound Healing
Scars: Clinical Evidence Base and Patient Impact
Skin: Histology and Physiology of Wound Healing
 Enhancement of Facial Scars With Dermabrasion
Laser Treatment for Improvement and Minimization of Facial Scars
Enhancement of Facial Scars With Dermabrasion
Laser Treatment for Improvement and Minimization of Facial Scars
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


