Scars after facial trauma or surgery can be a source of distress for patients, and facial plastic surgeons are frequently called upon to help manage them. Although no technique can remove a scar, numerous treatment modalities have been developed to improve facial scar appearance with varying levels of invasiveness. This article reviews techniques that camouflage scars without surgical intervention. Topical scar treatments, camouflage cosmetics, use of hairstyling and glasses, and facial prosthetics are discussed. In addition, professional counseling is provided on selection and application of topical cosmetics for use as part of an office practice.
- •
Although surgery inevitably produces a scar, patients have increasingly high expectations for minimally visible scarring.
- •
Good wound care including prevention of infection, moisturization, and minimal wound strain are critical to optimal scar formation.
- •
Petrolatum ointment remains the safest and most commonly used topical treatment during scar healing.
- •
Silicone has been shown to be effective in minimizing hypertrophic scars and is more effective as sheeting than as a gel.
- •
Vitamin A ointment may improve scars and reduce pruritis. Vitamin E ointment does not significantly improve scars and may be discouraged owing to sensitivity reactions.
- •
Other topical treatments, including Mederma, have not been shown to significantly improve scar appearance in clinical trials.
- •
Pressure dressings reduce hypertrophic scarring in burn wounds. Scar massage may improve pruritis and patient mood but has minimal effect on appearance.
- •
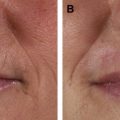
Camouflaging cosmetics come in a wide range of types for patient-specific uses, including minimizing discoloration and irregularities and creating an overall smooth facial appearance.
- •
Peripheral scarring may be adequately camouflaged by hairstyling, glasses, or facial hair.
- •
Facial prosthetics should be considered for craniomaxillofacial defects when surgical reconstruction is not the best option or needs to be delayed.
- •
Preoperative consultation with a craniomaxillofacial prosthetics center and trained anaplastologists assists in both surgical resection planning and facial prosthetics development.
The process of scar formation occurs as an important part of the healing process after damage to the skin’s dermal layer, whether through infection, trauma, or surgery. Although scars are both important and inevitable after injury, patients may find them functionally and cosmetically disruptive. Facial scars, in particular, are viewed as undesirable and potentially disfiguring. Research into the psychological effects of facial scarring has shown feelings of decreased self-worth, social self-consciousness, and isolation that persist after wound healing is complete. Distress over the persistence of facial scarring has been shown to have significant long-term quality of life impacts. However, patients also report lack of empathy from the medical community regarding scarring and poor long-term support services.
Facial plastic surgeons are frequently called upon to assist in the management of facial scarring. Although many techniques are present to minimize existing scars, none can erase a scar completely. Thorough explanation of inevitable scar development during consent for any surgical procedure is critical for patient understanding and satisfaction. With proper planning, minimization of scar development and camouflage of its appearance afterward can lead to satisfactory cosmetic outcomes without need for revision. In addition, both patients and physicians need to be aware of the many options available to them to reduce a scar’s appearance even after healing is complete.
This article reviews options for nonsurgical treatment of existing scars that can be used by the patient to improve a scar’s appearance. Treatments during the healing and maturation processes include occlusive dressings, topical treatments, and massage. Interventions for existing scar camouflage include topical cosmetics, use of hairstyling and glasses, and facial prosthetics. Descriptions of surgical planning and revision techniques, dermabrasion, laser resurfacing, and steroid injections are addressed in other articles (See the articles by William W. Shockley; Surowitz and Shockley; Foo and Tristani-Firouzi; Sobanko and Alster elsewhere in this issue for further exploration of this topic).
History of scar camouflage
A smooth flawless facial appearance is a primary determinant of health, youth, and beauty in many societies. For centuries, facial powders have been used to lighten and even the skin tone. However, powders do not hide scars well and require frequent reapplications. In seventeenth century Europe, beauty patches were used to cover and distract from disfiguring small pox scars. Facial foundation was later developed primarily for use in the theater to provide long-lasting skin coverage. The first true facial foundation was termed as wet white and incorporated white powder into a thin liquid base foundation. Grease paints were also developed to incorporate color and filler into an oil base for longer wear and coverage.
However, cosmetics continued to be the domain of the theater rather than the general public until Max Factor invented cake makeup in 1936. This compressed powder provided excellent coverage of skin irregularities with a lighter feel and more natural look than grease paints. In addition, the cake was carried in a convenient compact and easily applied with a damp sponge. Suddenly, facial foundation became convenient for the general public.
Since this time, the scope and application of modern facial foundations available has expanded dramatically. As a result, many patients now expect a flawless complexion and any scars to be minimally visible. However, no amount of surgical skill or scar revision can completely eliminate a scar. As a result, foundations have been improved for medical use, tattooing has expanded to include scar coverage, and medical teams have been developed for development of complex facial prosthetics. The modern facial plastic surgeon needs a working knowledge of the techniques available so that patients can make clear informed decisions on how to best camouflage their scar.
Topical scar treatment
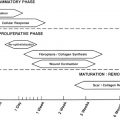
Scar healing requires several months before the final appearance is created. Early healing involves high levels of fibroblastic activity, which cause deposition of collagen. Erythema may present in the early stages from inflammation or neovascularization. Scars then mature over a period of several months, with the ideal scar being thin, level to surrounding skin, of good color match, and located along subunits or relaxed skin tension lines. Unfavorable scar formation results in noticeable color change, a depressed or raised scar, hypertrophy or keloid formation, or scar widening. Although some scar formation properties are genetic, knowledge of basic healing principles can reduce scar visibility. The surgeon is well aware of the importance of scar planning and meticulous closure techniques to eliminate tension and create skin eversion. However, postoperative care can affect scar formation while involving the patient in the healing process.
Wound Care
Control of concomitant medical issues and prevention of infection can aid in wound healing. Diabetic patients should closely monitor blood glucose levels. Patients who smoke should be counseled on the likelihood of more difficult healing and to reduce or quit smoking before surgery. Perioperative antibiotics are typically given to prevent infection, which greatly disrupts wound healing and is a predisposing factor for hypertrophic or keloid scars. Wounds should be kept clean with gentle removal of crusting and dirt using cotton swabs and peroxide. As necessary, the wound should be covered to prevent contamination or external trauma.
Dressings
In addition to keeping wounds clean, dressings can improve scar formation. Tape strips may reduce scar widening by preventing micromotion even in the mimetic facial muscles. Early consistent application of moisture through ointments or occlusive dressings aids in cell turnover and epidermal migration over the wound surface. Petroleum ointment is inexpensive and can be applied liberally without the risks of allergic reactions associated with antibiotic ointments.
Silicone
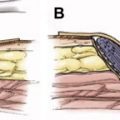
Silicone is the most rigorously studied topical scar improvement agent. In particular, silicone sheeting applied to wounds has been shown to improve wound healing and hypertrophic scar appearance. The silicone sheeting is thought to combine consistent pressure on the wound with an occlusive dressing that increases moisture in the stratum corneum. Doppler study of blood flow in scars with sheeting applied also indicates increased temperature that may assist in perfusion, although measurable blood flow changes are not seen. Silicone sheeting may be worn for 12 to 24 hours per day and may be rinsed and reapplied for up to 2 weeks. In addition, silicone applied as a topical gel has been shown to improve scars during the early healing phase by providing consistent moisture. Although not as effective on hypertrophic scar as sheeting, silicone gel has better patient compliance on visible areas such as the face.
Other Topicals
After initial wound healing and suture removal, patients may wish to apply a range of over-the-counter topical emollients. The most commonly available ointments include antioxidants such as retinoids (vitamin A) or tocols (vitamin E). Topical retinoic acid has been shown to both subjectively and objectively improve hypertrophic and keloid scar appearance. Vitamin E ointments, although commonly used by patients and even encouraged by some physicians, have not been shown to improve scar appearance. In another study, scar appearance worsened and local allergic reactions were noted, leading to discouragement of its use. Herbal extracts containing onions ( Allium cepa ) and madecassol ( Centella asiatica ) are also being aggressively marketed; studies have not demonstrated efficacy, but side effects are uncommon. One of the most marketed topical scar treatments Mederma (Merz Pharmaceuticals, Greensboro, NC, USA) is a gel-based onion extract that did not show significant improvement in scar healing or appearance in a randomized double-blinded split-scar study when compared with petroleum ointment.
Massage
Mechanical forces alone can have an effect on scar formation during the remodeling phase. Direct pressure has been shown to reduce inflammation and normalize hypertrophic scar composition and is used frequently in management of burn scars. Massage therapy has a long anecdotal history in management of hypertrophic scars. Most research has been performed in burn patients, in whom massage has been shown to improve pruritis, overall scar status, and patient depression levels. However, a prospective trial in pediatric burn patients with hypertrophic scarring failed to show a significant benefit of massage plus pressure dressing over pressure dressings alone on scar pliability and banding.
Topical scar treatment
Scar healing requires several months before the final appearance is created. Early healing involves high levels of fibroblastic activity, which cause deposition of collagen. Erythema may present in the early stages from inflammation or neovascularization. Scars then mature over a period of several months, with the ideal scar being thin, level to surrounding skin, of good color match, and located along subunits or relaxed skin tension lines. Unfavorable scar formation results in noticeable color change, a depressed or raised scar, hypertrophy or keloid formation, or scar widening. Although some scar formation properties are genetic, knowledge of basic healing principles can reduce scar visibility. The surgeon is well aware of the importance of scar planning and meticulous closure techniques to eliminate tension and create skin eversion. However, postoperative care can affect scar formation while involving the patient in the healing process.
Wound Care
Control of concomitant medical issues and prevention of infection can aid in wound healing. Diabetic patients should closely monitor blood glucose levels. Patients who smoke should be counseled on the likelihood of more difficult healing and to reduce or quit smoking before surgery. Perioperative antibiotics are typically given to prevent infection, which greatly disrupts wound healing and is a predisposing factor for hypertrophic or keloid scars. Wounds should be kept clean with gentle removal of crusting and dirt using cotton swabs and peroxide. As necessary, the wound should be covered to prevent contamination or external trauma.
Dressings
In addition to keeping wounds clean, dressings can improve scar formation. Tape strips may reduce scar widening by preventing micromotion even in the mimetic facial muscles. Early consistent application of moisture through ointments or occlusive dressings aids in cell turnover and epidermal migration over the wound surface. Petroleum ointment is inexpensive and can be applied liberally without the risks of allergic reactions associated with antibiotic ointments.
Silicone
Silicone is the most rigorously studied topical scar improvement agent. In particular, silicone sheeting applied to wounds has been shown to improve wound healing and hypertrophic scar appearance. The silicone sheeting is thought to combine consistent pressure on the wound with an occlusive dressing that increases moisture in the stratum corneum. Doppler study of blood flow in scars with sheeting applied also indicates increased temperature that may assist in perfusion, although measurable blood flow changes are not seen. Silicone sheeting may be worn for 12 to 24 hours per day and may be rinsed and reapplied for up to 2 weeks. In addition, silicone applied as a topical gel has been shown to improve scars during the early healing phase by providing consistent moisture. Although not as effective on hypertrophic scar as sheeting, silicone gel has better patient compliance on visible areas such as the face.
Other Topicals
After initial wound healing and suture removal, patients may wish to apply a range of over-the-counter topical emollients. The most commonly available ointments include antioxidants such as retinoids (vitamin A) or tocols (vitamin E). Topical retinoic acid has been shown to both subjectively and objectively improve hypertrophic and keloid scar appearance. Vitamin E ointments, although commonly used by patients and even encouraged by some physicians, have not been shown to improve scar appearance. In another study, scar appearance worsened and local allergic reactions were noted, leading to discouragement of its use. Herbal extracts containing onions ( Allium cepa ) and madecassol ( Centella asiatica ) are also being aggressively marketed; studies have not demonstrated efficacy, but side effects are uncommon. One of the most marketed topical scar treatments Mederma (Merz Pharmaceuticals, Greensboro, NC, USA) is a gel-based onion extract that did not show significant improvement in scar healing or appearance in a randomized double-blinded split-scar study when compared with petroleum ointment.
Massage
Mechanical forces alone can have an effect on scar formation during the remodeling phase. Direct pressure has been shown to reduce inflammation and normalize hypertrophic scar composition and is used frequently in management of burn scars. Massage therapy has a long anecdotal history in management of hypertrophic scars. Most research has been performed in burn patients, in whom massage has been shown to improve pruritis, overall scar status, and patient depression levels. However, a prospective trial in pediatric burn patients with hypertrophic scarring failed to show a significant benefit of massage plus pressure dressing over pressure dressings alone on scar pliability and banding.
Related posts:
 Proper Care of Early Wounds to Optimize Healing and Prevent Complications
Proper Care of Early Wounds to Optimize Healing and Prevent Complications
 Enhancement of Facial Scars With Dermabrasion
Enhancement of Facial Scars With Dermabrasion
 Skin: Histology and Physiology of Wound Healing
Scar Revision Techniques: Z-Plasty, W-Plasty, and Geometric Broken Line Closure
Skin: Histology and Physiology of Wound Healing
Scar Revision Techniques: Z-Plasty, W-Plasty, and Geometric Broken Line Closure
 Enhancement of Facial Scars With Dermabrasion
Laser Treatment for Improvement and Minimization of Facial Scars
Enhancement of Facial Scars With Dermabrasion
Laser Treatment for Improvement and Minimization of Facial Scars
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


