This article describes the physiology of wound healing, discusses considerations and techniques for dermabrasion, and presents case studies and figures for a series of patients who underwent dermabrasion after surgeries for facial trauma.
Dermabrasion is a well-established method of skin resurfacing, used for both facial rejuvenation and scar revision. The earliest known use of dermabrasion dates back to Egypt, 1500 BC, when sandpaper was used to revise scars. Many forms of skin resurfacing are available, including chemical peels, laser resurfacing, and mechanical resurfacing, known as dermabrasion . Dermabrasion results in the removal of the epidermis along with partial removal of the dermis. Dermabrasion devices consist of a powered hand piece and either a wire brush or diamond fraise. Although not viewed as “high tech” or glamorous, dermabrasion continues to be a popular adjunct to scar revision, with many benefits over other resurfacing options. As with any procedure, technical proficiency, experience, and understanding of its applications and limitations are paramount.
Physiology of wound healing
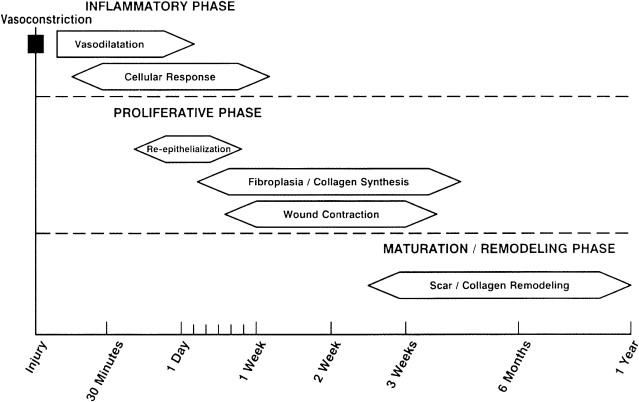
Understanding the physiology of wound healing is important when considering any skin resurfacing procedure. Wound healing occurs in progressive phases: the inflammatory phase, the proliferative phase, and the maturation phase; with significant overlap between the inflammatory and proliferative phases ( Fig. 1 ).
Inflammatory Phase
During the inflammatory phase, injury to endothelial cells results in exposure of subendothelial collagen, which acts as a binding surface for aggregation of platelets and results in their activation. The extrinsic and intrinsic coagulation cascades then occur, ultimately resulting in the activation of thrombin, which converts fibrinogen to fibrin. Fibrin then acts as the substrate for further platelet aggregation, migration of inflammatory cells, and plasma proteins. The inflammatory phase initially involves a period of vasoconstriction, mediated by epinephrine, norepinephrine, prostaglandins, serotonin, and thromboxane. This stage is followed by vasodilation, which is activated by histamines, prostaglandins, kinins, and leukotrienes. Macrophages function in phagocytosis and also release chemotactic and growth factors, including transforming growth factor (TGF)-β, basic fibroblast growth factor, epidermal growth factor, TGF-α, and platelet-derived growth factor, which is critical in endothelial cell and fibroblast proliferation.
Proliferative Phase
The proliferative phase begins within 24 hours of injury and has significant overlap with the inflammatory phase. Epithelial regeneration, fibroplasia, collagen formation, wound contraction, and neovascularization all occur during the proliferative phase. Epithelial regeneration begins within 24 hours of injury and is at its peak between 48 and 72 hours. Reepithelialization occurs as a result of the migration of epithelial cells from the wound margins and from within adnexal structures of the skin, which include sweat glands, hair follicles, and sebaceous glands. Basal stem cells within the adnexae undergo differentiation and subsequent migration, which is why it is paramount to dermabrade only down as far as the superficial reticular dermis, otherwise epithelialization will be impaired and scarring may result ( Fig. 2 ). Apposition of advancing epithelial cells results in inhibition of further migration, and in stratification and differentiation.
Related posts:
 Use of Makeup, Hairstyles, Glasses, and Prosthetics as Adjuncts to Scar Camouflage
Use of Makeup, Hairstyles, Glasses, and Prosthetics as Adjuncts to Scar Camouflage
 Use of Hair Grafting in Scar Camouflage
Use of Hair Grafting in Scar Camouflage
 Enhancement of Facial Scars With Dermabrasion
Enhancement of Facial Scars With Dermabrasion
 Scars: Clinical Evidence Base and Patient Impact
Scars: Clinical Evidence Base and Patient Impact
 Keloids: Prevention and Management
Laser Treatment for Improvement and Minimization of Facial Scars
Keloids: Prevention and Management
Laser Treatment for Improvement and Minimization of Facial Scars
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


